kottke.org posts about Covid-19
In popular press and social media, there’s been a misunderstanding of what is actually meant when scientists say that the Pfizer and Moderna Covid-19 vaccines have an efficacy of 94-95%. It does not mean that 95% of vaccinated people are protected from infection — these vaccines are better than that. Dr. Piero Olliaro explains in a letter to The Lancet:
The mRNA-based Pfizer and Moderna vaccines were shown to have 94-95% efficacy in preventing symptomatic COVID-19, calculated as 100 x (1 minus the attack rate with vaccine divided by the attack rate with placebo). It means that in a population such as the one enrolled in the trials, with a cumulated COVID-19 attack rate over a period of 3 months of about 1% without a vaccine, we would expect roughly 0.05% of vaccinated people would get diseased.
Another way to put it: you’re 20 times less likely to get Covid-19 with a vaccine than without. (And again, data indicates these are safe vaccines.) Olliaro explains with some simple math:
If we vaccinated a population of 100,000 and protected 95% of them, that would leave 5000 individuals diseased over 3 months, which is almost the current overall COVID-19 case rate in the UK. Rather, a 95% vaccine efficacy means that instead of 1000 COVID-19 cases in a population of 100,000 without vaccine (from the placebo arm of the abovementioned trials, approximately 1% would be ill with COVID-19 and 99% would not) we would expect 50 cases (99.95% of the population is disease-free, at least for 3 months).
And of course if you vaccinate widely, it becomes a compounding situation because the virus just runs out of people to infect.
Over the past week or two, I’ve read a number of articles and threads about why Covid-19 cases are falling so rapidly in the US. The explanations have all been somewhat unsatisfying to me. Cases have indeed dropped off quite quickly and it happened pretty uniformly all over the country. Look at the mini state graphs on the NY Times Covid page — they all look about the same. Hospitalizations and positivity rates have dropped too, so while the number of daily tests has fallen too, this appears to be a real drop and not just an artifact of a lack of testing. Which is great news! Imagine a February and March that looked like December — a disaster compounded.
So what’s going on here? For The Atlantic, Derek Thompson lists four reasons for the decline in cases and hospitalizations that mirror the arguments I’ve seen elsewhere: “social distancing, seasonality, seroprevalence, and shots”.
The vaccine explanation is the weakest one for me: not enough people outside of healthcare workers had gotten them early enough to start bending that curve sharply downward in early January. But as Thompson notes, it could be having more of an effect on hospitalizations because the folks getting shots (and therefore immunity against severe infection) are those most likely to end up in hospitals due to infection. And obviously, vaccines are going to become the dominant factor in falling case numbers as more and more people get jabbed.
I’m also skeptical of the seasonality argument, but (again, as Thompson notes) there’s a lot we don’t know about how temperature, sunlight, humidity, and this specific coronavirus interact. Obviously Covid-19 is a seasonal thing and that’s definitely a contributing factor here, but that sharp of a drop in early January? I don’t know if it’s the primary driver here. Also, the seasonal flu typically peaks in February in the US.
The seroprevalence argument is an interesting one. Here’s Johns Hopkins infectious disease epidemiologist David Dowdy in a great Twitter thread about the US case decline:
I think the most logical explanation is one proposed initially by @mgmgomes1 and others — namely that we are seeing the effects of population immunity with heterogeneous mixing + strong behavioral effects. Take a(n overly) simple example. Assume 60% of a population has zero respiratory contacts, while the other 40% lives life as normal. If 75% of that high-mixing group has immunity (e.g., 30% population seroprevalence), you could easily see herd effects.
Basically, a large percentage of the folks at the greatest risk of getting Covid-19 in the US (i.e. folks who aren’t able or willing to keep from seeing other people and/or take proper precautions) have gotten it, resulting in a sort of localized “herd immunity” among those folks. After the massive holiday surge in cases (more on that in a sec), this hypothesis suggests, the virus started running out of people to infect and rates dropped quickly. This is the first explanation I read that really made sense to me.
Thompson leads off his piece with the behavioral explanation: “Maybe Americans finally got the hang of this mask and social-distancing thing.” I do not buy that people who previously weren’t doing so before suddenly started wearing masks (or better masks), keeping distant, spending less time indoors with others, and staying home from work started doing so in numbers large enough to cause such a sharp downturn. But you can’t consider the decline without also looking at how cases got so high in the first place. Here’s Steven Johnson on Twitter, zooming out a few months:
[It’s] not so much that people got the hang of social distancing, but rather that the holiday season compelled people to relax social distancing for in-person family gatherings. So the current decline is mostly reversion to where we were in Oct-Nov.
Yes, this. Without these holidays, we may have seen much more of a winter plateau than a spike. So here’s what seems plausible to me. As the cold weather made the coronavirus more effective at infection, people gathered for Halloween, Thanksgiving, Hanukkah, Christmas, and New Year’s — each subsequent holiday building on the previous one — and it pushed cases much higher than they would have been without those major gatherings. After two months of massive infection rates, the virus burned itself out among the high-mixing group and everyone else retreated back into their homes and pods to hunker down, resulting in the steep decline we’re seeing.
Obviously, careful scientific study will be necessary to tease out how significant each of these (and other!) causes were to the holiday spike and subsequent decline. But for now, the way forward is continuing to social distance, wear (better) masks, limit close contacts, and get people vaccinated — before B.1.1.7 and the other variants hit.
This guide to Covid-19 variants (SARS-CoV-2 viruses that have evolved changes to meaningfully alter their behavior) by Michaeleen Doucleff and Meredith Rizzo at NPR cleverly visualizes how mutations of the virus’s spike proteins help bind it more easily to ACE2 receptors on human cells. The key to the visualization is Meredith Miotke’s illustrations of the viruses using Lego pieces to represent the virus spikes and cell receptors. The usual SARS-CoV-2 has 1x1 Lego pieces that can bind with 1x2 pieces, like so:
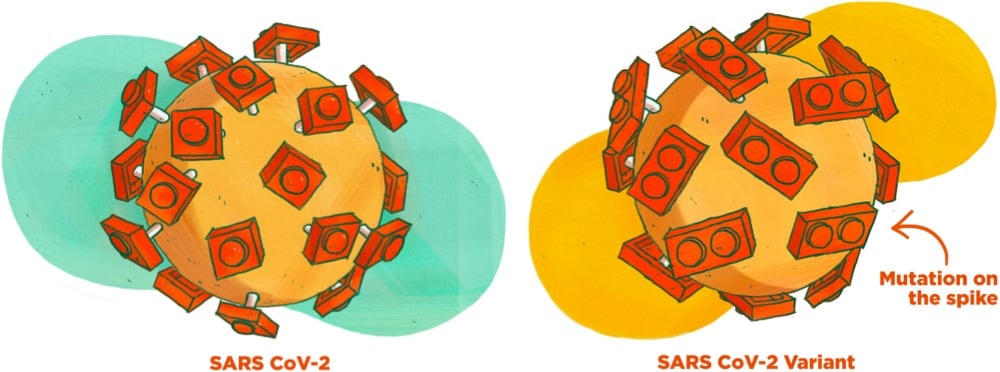
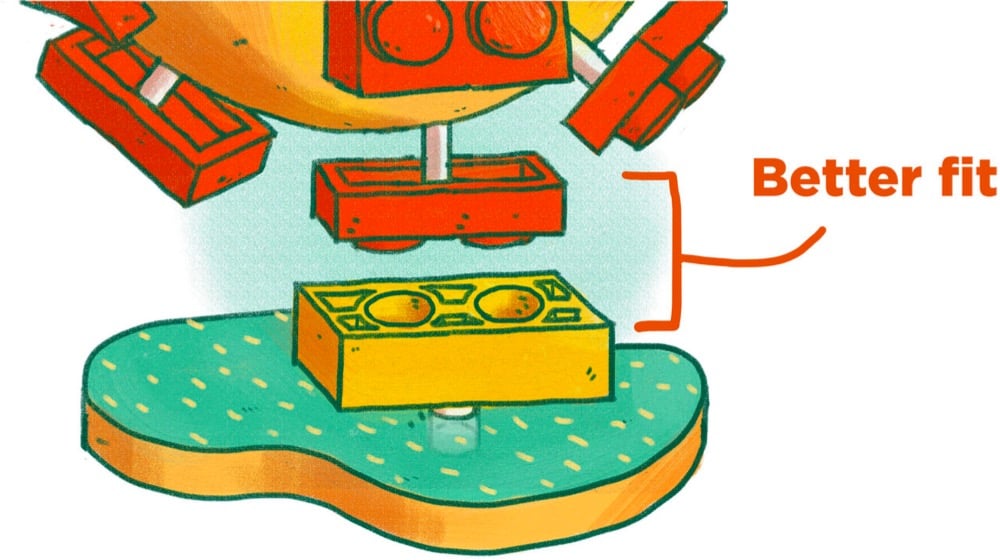
But, as everyone who has ever worked with a Lego set knows, a 1x1 piece stuck to a 1x2 piece is not super stable. So when a version of the virus with a 1x2 piece shows up, it’s able to form a better connection to the 1x2 receptor:
The analogy breaks down if you look too hard at it1 but for many people, it can be a quick way to get the gist of the mechanism at work here. (via @EricTopol)
Concerned that recent articles like this one about screen time panic were not adequately capturing the perspective of the kids themselves, Anne Helen Petersen asked a group of parents and caregivers to conduct interviews with kids about gaming and screen time.
So I wanted to hear them talk about their own relationship to the games they play: what they like about it, when they like to play, how games make them feel, who they like to play with, and how they respond to anxiety about their gaming/screen time.
I pulled out a few quotes from the kids but the whole thing is worth a read.
When people say that screentime is bad, I want to say, hey, I want to be more social at the moment and it’s hard to do that right now and I can only do it with technology.
I feel annoyed and angry with the “too much time playing video games argument,” because people don’t really understand. They don’t play these games. They don’t have any experience themselves, and they’re judging what we do based on what they’ve heard or read. Gaming is so new that there’s no conclusive evidence yet to prove if it’s actually harmful. It feels like they’re just trying to control us and tell us what to do.
When adults say that kids play too many video games it makes me kinda angry and confused. We’re already stuck at home and it feels like they’re trying to cut us off from our friends even more. So it’s kinda annoying.
Honestly I don’t really worry about spending too much time game at all. I already spend almost all my time on there anyway and it doesn’t seem to have any negative side effects. Key word “seem.” People need to make sure they don’t get correlation and causation mixed together.
Like many other parents, we’ve been struggling mightily with games, devices, and screen time during the pandemic (although for us this is an issue that carried over from The Before Times). As Petersen says, this is a complicated challenge and I am sympathetic to both the arguments these kids make (which mirror what I’ve heard from my kids) and parental concerns about too much time on devices (the effects of which I’ve seen in my kids).
What we’ve done, imperfectly, is prioritize the social aspect of gaming time — playing with friends, gaming clubs, playing together in the living room — over manically grinding away for hours on end in a dark room. We try to meet them on their terms — ask them what they did today in Minecraft or Among Us, show real interest about their progress, etc. I empathize and commiserate when I can — I grew up playing video games and I still get a little too into them on my phone or iPad sometimes. But we also encourage them to get outside and move their bodies, find ways to connect with friends that don’t involve killing virtual people, and try to get them to recognize some of the worst effects of too much screen time (they do, if you catch them at the right moment about it). Keeping a good connection with your kids around gaming & screens is the key bit, I think. With that in hand, in theory it’s at least possible to keep kids and parents alike safe and sane during all of this.

You probably read something yesterday, maybe just a headline, about Moderna’s Covid-19 vaccine being “six times less effective” against the B.1.351 coronavirus variant first identified in South Africa. This is, to put it plainly, a bullshit take on what is actually excellent news. This is the important bit, via Stat:
Both the Moderna vaccine and the immunization from Pfizer-BioNTech produce such powerful levels of immune protection — generating higher levels of antibodies on average than people who recover from a Covid-19 infection have — that they should be able to withstand some drop in their potency without really losing their ability to guard people from getting sick.
“There is a very slight, modest diminution in the efficacy of a vaccine against it, but there’s enough cushion with the vaccines that we have that we still consider them to be effective,” Anthony Fauci, the top U.S. infectious diseases official, said Monday on the “Today” show.
Let’s hear that again: “Both the Moderna vaccine and the immunization from Pfizer-BioNTech produce such powerful levels of immune protection…” These vaccines are so good, so potent, that even this sixfold drop in one measure of the vaccines’ ability to neutralize this one SARS-CoV-2 variant isn’t even enough to significantly reduce their overall protective power.1 That’s the important news here, that’s the very good news, that’s what you should be taking away from this. We have miraculously developed a near-perfect medicine for a plague that has significantly disrupted all human life on Earth and we’re flipping out over some technical details that the experts assure us don’t mean much in terms of overall effectiveness?! No thank you. Not today.
In a Twitter thread, Zeynep Tufekci is tearing her hair out because of the media’s misunderstanding and sensationalization of the “sixfold drop”.
I know people are tired but needless anxiety isn’t helping us. Let’s focus on getting through these months — better masks if indoors with others, more strict attention to our precautions — and the real problem: making more of these amazing vaccines quickly & getting them out there!
I get it, we want to understand but not how it works. Stop worrying about Nab titers. That does NOT mean the vaccine is six times less effective. People whose job it is to worry about it are on it & we just got confirmation: it works against the variants.
Plea to media: this isn’t a good headline. It makes people think the vaccine is six times less effective against the new variants (FALSE!) when the news today is *excellent*: The vaccine continues to work well against the new variants. That’s the headline.
For a much more technical take on the efficacy of the vaccines against variants, see virologist Florian Krammer’s long thread. His conclusion:
mRNA vaccines induce very high neutralizing antibodies after the second shot (consistently in the upper 25-30% of what we see with convalescent sera). If that activity is reduced by 10-fold, it is still decent neutralizing activity that will very likely protect. Furthermore, we know that the mRNA vaccines are already protective after the first shot when neutralizing antibody titers are low or undetectable in most individuals.
There is a concern here and it’s that B.1.351 or B.1.1.7 might mutate into variants that are significantly resistant against the vaccines’ good effects. Krammer again:
First, we need to do what every good scientist is praying for a year now: We need to cut down on virus circulation. The more the virus replicates, the more infections there are the higher are the chances for new variants to arise. Also, we need to try and contain B.1.351 and B.1.1.248/P.1 as much as possible.
That’s why, aside from preventing hundreds of thousands of deaths in the next several months, getting these vaccines into people’s arms is so important: the less the virus spreads, the less opportunity it will have to mutate into something even more dangerous. The US vaccination effort is slowly ramping up — we’re at an average of 1.3 million doses per day right now and the trend is heading in the right direction. We can get this done!
So what can you do about this right now? 1. Stop worrying about the variants until the experts let us know we have something to worry about. 2. If you are eligible for the vaccine, get it! 3. Spread the word about vaccine availability in your area. Yesterday Vermont opened signups for vaccination appointments for all Vermonters 75 and older, and I texted/emailed everyone I could think of who was over 75 or who had parents/relatives/friends who are over 75 to urge them to sign up or spread the word. 4. Continue to wear a mask (a better one if possible), wash your hands, social distance, stay home when possible, don’t spend time indoors w/ strangers, etc. Thanks to these remarkable vaccines, real relief is in sight — let’s keep on track and see this thing through.
With tongue in cheek, Jon Methven writes about what it’s like to take a walk during the pandemic.
My knapsack is full. I’ve stowed backup masks should I encounter any maskless pandemic denialists. I have Band-Aids, cotton balls and large-wound bandages, in case my run-in with the anti-maskers goes awry. I packed five gallons of backup sanitizer and a refill funnel. I have nine factory-sealed packages of antiseptic wipes. I packed face shields and oral swabs and disposable thermometers in case I need to self-test. I have a rolling oxygen tank. This jaunt is just what I need to unwind.
At least now people without kids know what it’s like leaving the house with a toddler.
In response to comments about a video of him getting the Covid-19 vaccine — “Come with me if you want to live!” — Arnold Schwarzenegger says that if you want to build biceps, you should listen to him. He’s the expert. But if you want to know what to do about Covid-19, you should listen to epidemiologists and doctors.
Dr. Fauci and all of the virologists and epidemiologists and doctors have studied diseases and vaccines for their entire lives, so I listen to them and I urge you to do the same. None of us are going to learn more than them by watching a few hours of videos. It’s simple: if your house is on fire, you don’t go on YouTube, you call the damn fire department. If you have a heart attack, you don’t check your Facebook group, you call an ambulance. If 9 doctors tell you you have cancer and need to treat it or you will die, and 1 doctor says the cancer will disappear, you should always side with the 9. In this case, virtually all of the real experts around the world are telling us the vaccine is safe and some people on Facebook are saying it isn’t.
In general, I think if the circle of people you trust gets smaller and smaller and you find yourself more and more isolated, it should be a warning sign that you’re going down a rabbit hole of misinformation. Some people say it is weak to listen to experts. That’s bogus. It takes strength to admit you don’t know everything. Weakness is thinking you don’t need expert advice and only listening to sources that confirm what you want to believe.
On his blog, Conor Barnes shared an eclectic list of 100 Tips For A Better Life. I’m less keen on these sorts of lists than I used to be because they’re often written for people who already have pretty good lives and it’s too easy to imagine that a list advocating the opposite of each tip would also lead to a better life. To be fair, Barnes’ list acknowledges the difficulty with generalized advice:
31. The best advice is personal and comes from somebody who knows you well. Take broad-spectrum advice like this as needed, but the best way to get help is to ask honest friends who love you.
That said, here are some of the list items that resonated with me in some way.
3. Things you use for a significant fraction of your life (bed: 1/3rd, office-chair: 1/4th) are worth investing in.
I recently upgraded my mattress from a cheap memory foam one I’d been using for almost 7 years to a hybrid mattress that was probably 3X the cost but is so comfortable and better for my back.
13. When googling a recipe, precede it with ‘best’. You’ll find better recipes.
I’ve been doing this over the past year with mixed results. Google has become a terrible way to find good recipes, even with this trick. My version of this is googling “kenji {name of dish}” — works great.
27. Discipline is superior to motivation. The former can be trained, the latter is fleeting. You won’t be able to accomplish great things if you’re only relying on motivation.
My motivation is sometimes very low when it comes to working on this here website. But my discipline is off the charts, so it gets done 99 days out of 100, even in a pandemic. (I am still unclear whether this is healthy for me or not…)
46. Things that aren’t your fault can still be your responsibility.
48. Keep your identity small. “I’m not the kind of person who does things like that” is not an explanation, it’s a trap. It prevents nerds from working out and men from dancing.
Oh, this used to be me: “I’m this sort of person.” Turns out, not so much.
56. Sometimes unsolvable questions like “what is my purpose?” and “why should I exist?” lose their force upon lifestyle fixes. In other words, seeing friends regularly and getting enough sleep can go a long way to solving existentialism.
75. Don’t complain about your partner to coworkers or online. The benefits are negligible and the cost is destroying a bit of your soul.
Interpreting “partner” broadly here, I completely agree with this one. If they are truly a partner (romantic, business, parenting), complaining is counterproductive. Instead, talk to others about how those relationships can be repaired, strengthened, or, if necessary, brought to an appropriate end.
88. Remember that many people suffer invisibly, and some of the worst suffering is shame. Not everybody can make their pain legible.
91. Human mood and well-being are heavily influenced by simple things: Exercise, good sleep, light, being in nature. It’s cheap to experiment with these.
This is good advice, but some of these things actually aren’t “cheap” for some people.
100. Bad things happen dramatically (a pandemic). Good things happen gradually (malaria deaths dropping annually) and don’t feel like ‘news’. Endeavour to keep track of the good things to avoid an inaccurate and dismal view of the world.
Oof, this ended on a flat note. Many bad things seem to happen dramatically because we don’t notice the results of small bad decisions accumulating over time that lead to sudden outcomes. Like Hemingway said about how bankruptcy happens: gradually, then suddenly. Lung cancer doesn’t happen suddenly; it’s the 40 years of cigarettes. California’s wildfires are the inevitable result of 250 years of climate change & poor forestry management techniques. Miami and other coastal cities are being slowly claimed by the ocean — they will reach breaking points in the near future. Even the results of something like earthquakes or hurricanes can be traced to insufficient investment in safety measures, policy, etc.
The pandemic seemed to come out of nowhere, but experts in epidemiology & infectious diseases had been warning about a pandemic just like this one for years and even decades. The erosion of public trust in government, the politicization of healthcare, the deemphasis of public health, and the Republican death cult (which is its own slow-developing disaster now reaching a crisis) controlling key aspects of federal, state, and local government made the pandemic impossible to contain in America. (This is true of most acute crises in the United States. Where you find people suffering, there are probably decades or even centuries of public policy to blame.)
Bad news happens slowly and unnoticed all the time. You don’t have to look any further for evidence of this than how numb we are to the fact that thousands of Americans are dying every single day from a disease that we know how to control. So, endeavour to keep track of the bad things to avoid an inaccurate and unrealistically optimistic view of the world — it helps in making a list of injustices to pay attention to and work against.
In an opinion piece for the NY Times, Zeynep Tufekci and epidemiologist Michael Mina are urging for new trials of the Moderna and Pfizer/BioNTech Covid-19 vaccines to begin immediately to see how effective a single dose might be in preventing new infections. If the trials do indicate that a single dose works, that would effectively double the number of people we could vaccinate within a certain time period, saving countless lives in the US and worldwide.
Both vaccines are supposed to be administered in two doses, a prime and a booster, 21 days apart for Pfizer and 28 days for Moderna. However, in data provided to the F.D.A., there are clues for a tantalizing possibility: that even a single dose may provide significant levels of protection against the disease.
If that’s shown to be the case, this would be a game changer, allowing us to vaccinate up to twice the number of people and greatly alleviating the suffering not just in the United States, but also in countries where vaccine shortages may take years to resolve.
But to get there — to test this possibility — we must act fast and must quickly acquire more data.
For both vaccines, the sharp drop in disease in the vaccinated group started about 10 to 14 days after the first dose, before receiving the second. Moderna reported the initial dose to be 92.1 percent efficacious in preventing Covid-19 starting two weeks after the initial shot, when the immune system effects from the vaccine kick in, before the second injection on the 28th day
That raises the question of whether we should already be administrating only a single dose. But while the data is suggestive, it is also limited; important questions remain, and approval would require high standards and more trials.
The piece concludes: “The possibility of adding hundreds of millions to those who can be vaccinated immediately in the coming year is not something to be dismissed.”
In remarks to the German parliament today, German Chancellor Angela Merkel advocated for tighter Covid-19 restrictions, as cases & deaths in Germany reach new peaks. The restrictions she’s referring to were recommended by “a national academy of scientists and academics” and are intended at reducing the spread of Covid-19 over the December holidays. The impassioned argument that she makes in this short video clip (full report here) is difficult for me to find fault with (even though conservative members of her parliament and Twitter commenters disagree). Here’s a partial transcript:
If the price we pay is 590 deaths per day, then that is unacceptable in my view. And when scientists are practically begging us to reduce our contacts for a week before we see Grandma and Grandpa, grandparents and older people at Christmas, then perhaps we really should think again about whether we can’t find a way to start the school holidays on the 16th instead of the 19th. What will we say when we look back on this once-in-a-century event if we weren’t able to find a solution for these three days? And it may be the case that sending children home is the wrong thing to do, if so then it will have to be digital lessons or something else. I don’t know, this is not my area of expertise and I don’t want to interfere. I only want to say: if we have too many contacts now, in the run-up to Christmas, and it ends up being the last Christmas with our grandparents, then we will have done something wrong. She should not let this happen.
I teared up watching her talk. In the US, we are dealing with many more cases (which will turn into eventual deaths) and deaths than Germany, both in absolute and per capita terms. It’s like 10 fully-loaded passenger planes a day are crashing with no survivors and there are small things that we all can do to keep many of those people alive and … many of us just don’t want to do those things!
Like Merkel says, we are going to look back on this and be completely ashamed that we didn’t do these things and that we elected people that won’t advocate for these things on our behalf and that we let 300-400,000 Americans die and countless others lose loved ones and go bankrupt and get evicted and lose their businesses and be chronically ill and be food insecure and and and. If we aren’t ashamed, if we don’t reckon with all of this someday, then maybe nothing can redeem us and we deserved it all.
The Kottke Ride Home podcast has been humming away since August and host Jackson Bird has been sharing some great stuff lately. From today’s show comes this New York magazine piece by David Wallace-Wells about the stunning speed with which the Covid-19 vaccine was developed:
You may be surprised to learn that of the trio of long-awaited coronavirus vaccines, the most promising, Moderna’s mRNA-1273, which reported a 94.5 percent efficacy rate on November 16, had been designed by January 13. This was just two days after the genetic sequence had been made public in an act of scientific and humanitarian generosity that resulted in China’s Yong-Zhen Zhang’s being temporarily forced out of his lab. In Massachusetts, the Moderna vaccine design took all of one weekend. It was completed before China had even acknowledged that the disease could be transmitted from human to human, more than a week before the first confirmed coronavirus case in the United States. By the time the first American death was announced a month later, the vaccine had already been manufactured and shipped to the National Institutes of Health for the beginning of its Phase I clinical trial.
Monday’s show featured the intrigue behind the discovery of a real life treasure:
And if you look back to last week, Jackson clued us in to Radiooooo (“The Musical Time Machine”), Tetris championships, China’s Chang’e 5 mission to the Moon, and DeepMind’s AI breakthrough in protein folding.
If any or all of that sounds interesting to you, you can subscribe to Kottke Ride Home right here or in your favorite podcast app.
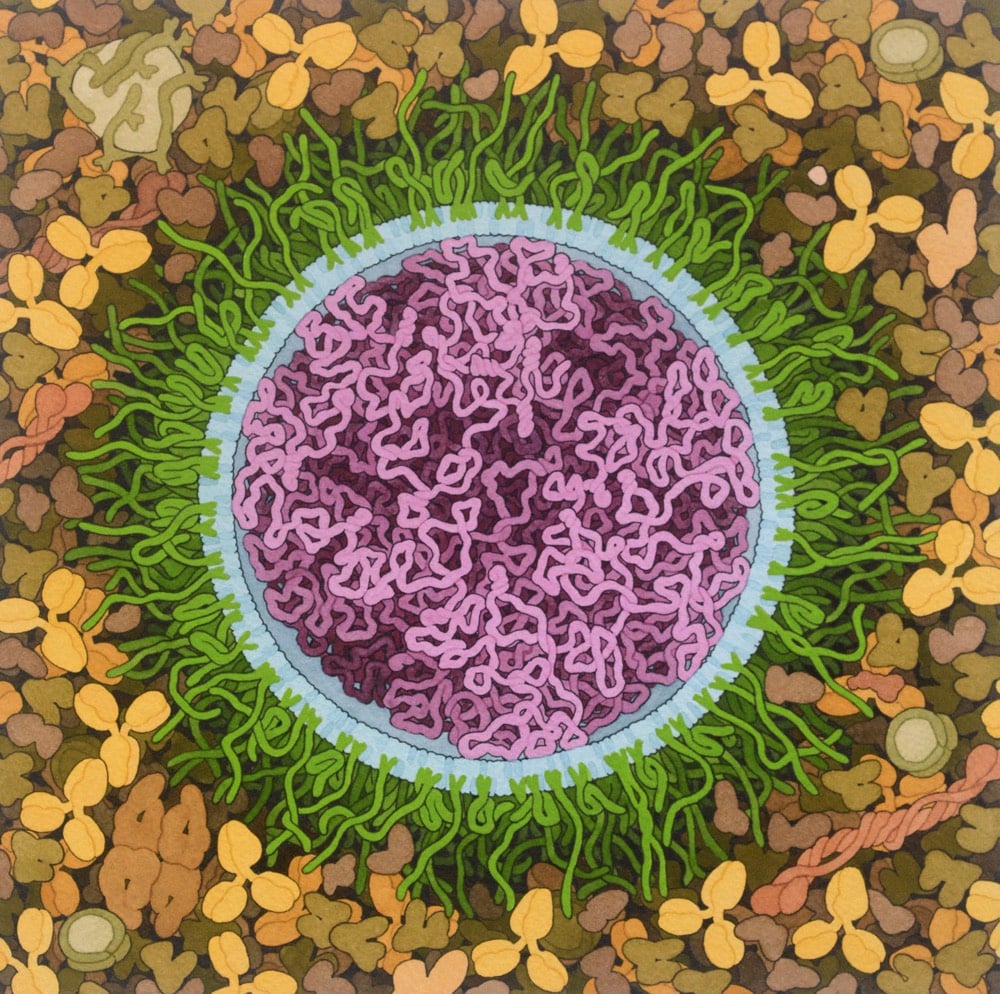
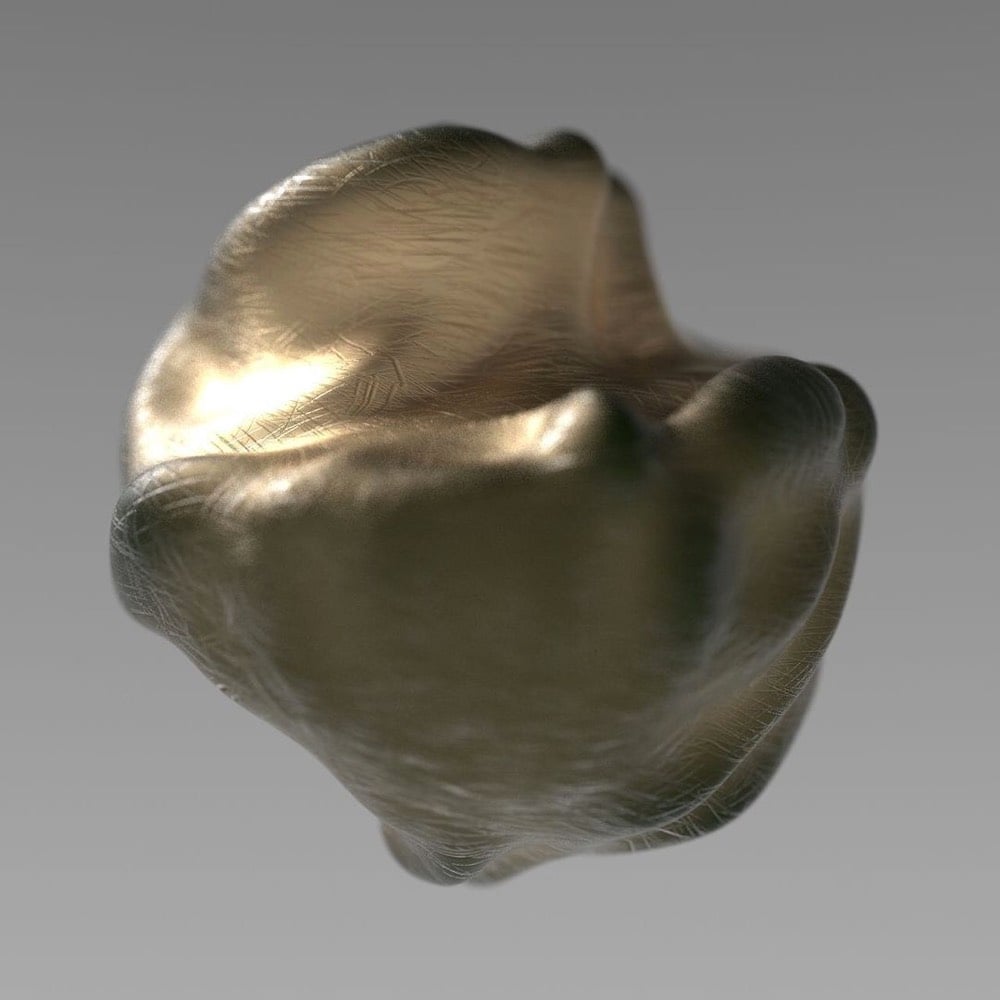
Artist and biologist David Goodsell has done a painting of the Covid-19 mRNA vaccine.
The vaccine structure is highly idealized, with spike mRNA in magenta, lipids in blue, and PEG-lipid in green. The background is blood serum or lymph.
Both the Pfizer/BioNTech and the Moderna Covid-19 vaccines are based on mRNA — you can brush up on how they work at Stat or the CDC.
mRNA vaccines are a new type of vaccine to protect against infectious diseases. To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, they teach our cells how to make a protein — or even just a piece of a protein — that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.
See also Goodsell’s painting of a SARS coronavirus from back in February.
The NY Times recently surveyed 700 epidemiologists about how they are personally living during the pandemic and what they think is going to happen next. Epidemiologists should have a better idea than most of us about how to act during a viral pandemic, so there’s lots of good information in there about vaccines and high-risk behaviors. But I found their answers to a pair of speculative questions about a return to normalcy most interesting.
How and when will life go back to normal?
“For some, it has gone back to normal, and because of this, it will be two to three years before things are back to normal for the cautious, at least in the U.S.”
- Cathryn Bock, associate professor, Wayne State University
“The new normal will be continued masking for the next 12 to 18 months and possibly the next few years. This is a paradigm shift.”
- Roberta Bruhn, co-director, Vitalant Research Institute
What will never return to normal?
“My relationships with people who have taken this pandemic lightly and ignored public health messages and recommendations.”
- Victoria Holt, professor emeritus, University of Washington
“Every part of my daily life that involves interaction with anyone other than my spouse.”
- Charles Poole, associate professor, University of North Carolina
For many people, the pandemic has altered almost every aspect of their lives. If we listen to what epidemiologists are telling us (like we should have back in early 2020 to avoid much of our present hardship), it could help us accept that the pandemic will continue to affect most aspects of our lives even after it is “over”.
Free Covid-19 illustration courtesy of Pixel True.
Zeynep Tufekci reports on a small study from Korea that has big implications on how we think about transmission of SARS-CoV-2. Scientists traced two cases back to a restaurant and discovered that transmission had occurred over quite a long distance in a very short period of time.
If you just want the results: one person (Case B) infected two other people (case A and C) from a distance away of 6.5 meters (~21 feet) and 4.8m (~15 feet). Case B and case A overlapped for just five minutes at quite a distance away. These people were well beyond the current 6 feet / 2 meter guidelines of CDC and much further than the current 3 feet / one meter distance advocated by the WHO. And they still transmitted the virus.
As Tufekci goes on to explain, the way they figured this out was quite clever: they contact traced, used CCTV footage from the restaurant, recreated the airflow in the space, and verified the transmission chain with genome sequencing. Here’s a seating diagram that shows the airflow in relation to where everyone was sitting:
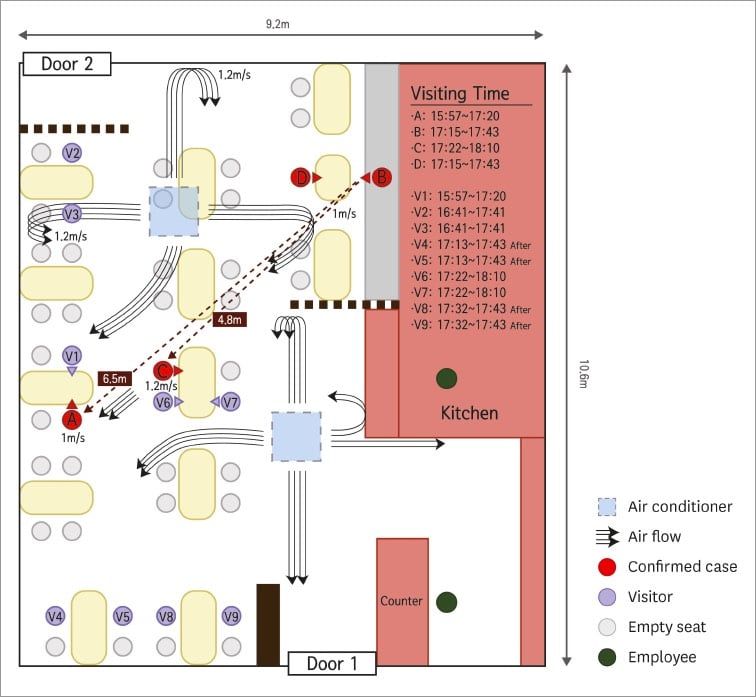
Someone infecting another person 21 feet away in only five minutes while others who were closer for longer went uninfected is an extraordinary claim and they absolutely nailed it down. As Sherlock Holmes said: “Once you eliminate the impossible, whatever remains, no matter how improbable, must be the truth.” And the truth is that in some cases, the recommended 6 feet of distance indoors is not sufficient when people aren’t wearing masks. Airflow matters. Ventilation matters. Which way people are facing matters. How much people are talking/laughing/yelling/singing matters. Masks matter. 6 feet of distance does not confer magical protection. All that can make it tough to figure out if certain situations are safe or not, but for me it’s an easy calculation: absolutely no time indoors with other people not wearing masks. Period. As Tufekci concludes:
I think there are three broad lessons here. One, small data can be extremely illuminating. Two, air flow and talking seem to matter a great deal. Three, sadly, indoor dining and any activity where people are either singing or huffing and puffing (like a gym) indoors, especially with poor ventilation, clearly remains high risk.
Read her whole post — as she says, it’s “perhaps one of the finest examples of shoe-leather epidemiology I’ve seen since the beginning of the pandemic”.
With the first approved Covid-19 vaccines set to roll out in the US soon, some of the focus has shifted to how the vaccine will be distributed and its equitable allocation. Part of the distribution logistics puzzle is making sure there are enough glass vials to hold and transport the vaccine around the nation to those waiting to be vaccinated. For the New Yorker, Christopher Payne took some photos of two Corning factories that are manufacturing vials as fast as they can.
But back in the early 19th century, for a colonial empire dealing with overseas smallpox epidemics, glass vials were not an option. Smallpox vaccination at that time was most reliably accomplished by transferring material from cowpox blisters on one person (or cow) to another person. The freshly inoculated person got a little sick but later proved to be immune to the much deadlier smallpox. So when Spain’s Royal Philanthropic Vaccine Expedition set sail in 1803 to inoculate the inhabitants of their overseas colonies for smallpox, they used the bodies of human beings to transport the vaccine. To be more specific, they used “twenty-two orphan boys, ages three to nine”.1
And so it was that, “in the era before refrigeration, freeze-dried vaccines, and jet aircraft,” writes medical historian John Bowers, “the successful circumnavigation of the globe with the vaccine…rested on a single medium — little boys.” During the long crossing, approximately twenty-two orphans who had not previously contracted smallpox or cowpox were “vaccinated in pairs every ninth or tenth day,” via arm-to-arm inoculation (taking lymph from an unbroken pustule on a recently vaccinated boy and introducing it under the skin of another). This created a vaccine chain — the vaccine remained active and viable for the entire journey.
The three-year expedition was success and an early & effective example of philanthropic healthcare, but you also have to note here that the reason the Americas were ravaged by smallpox was because Spain brought it there in the first place.
Update: In The Atlantic, Sam Kean provides some more detail on the vaccination effort.
Given the era, it’s likely that no one asked the orphans whether they wanted to participate — and some seemed too young to consent anyway. They’d been abandoned by their parents, were living in institutions, and had no power to resist. But the Spanish king, Carlos IV, decided to make them a few promises: They would be stuffed with food on the voyage over to make sure they looked hearty and hale upon arrival. After all, no one would want lymph from the arm of a sickly child. Appearance mattered. And they’d get a free education in the colonies, plus the chance at a new life there with an adoptive family. It was a far better shake than they’d get in Spain.
In an incredible effort, science has provided the world with what looks like an incredibly effective vaccine for Covid-19. For Stat, Helen Braswell writes about the challenges of turning that vaccine into vaccinations. In the US, despite heroic work from individuals and individual groups, our public health system has proved unequal to the challenge of addressing the pandemic, and we’re now turning, in part, to that system to distribute and administer the vaccines, as well as to educate the public and drum up support for vaccination. The people that we’re counting on are public officials and healthcare workers worn out from what is essentially one 9-month-long wave of illness, hospitalizations, and death across the country. Misinformation and skepticism of science and government has sowed “justified distrust” about vaccines in many people:
Concern about the vaccines, however, cuts across ethnic and socioeconomic groups. President Trump’s overt efforts to pressure the FDA to issue EUAs before the Nov. 3 election — before the vaccine trials were finished — has deepened the sense of unease. The CDC’s early pandemic testing fiasco, coupled with its sidelining by the Trump administration, has eroded its standing as a trusted source of information.
Alison Buttenheim, an associate professor of nursing and health policy at the University of Pennsylvania, refers to the current situation as a perfect storm of “justified distrust.”
“People who don’t think twice about vaccinating their kids totally on time, who get their flu shot every year, are in the sort of, ‘Hmmm. Might wait six months on this one,’” Buttenheim, who works on vaccine acceptance, told STAT. “I’ve heard people say, ‘I’ll get the European one,’” she said, adding other people have said they would get vaccinated after Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, gets vaccinated.
And it’s not just the general public. A recent survey of 2,000 doctors and nurses in New Jersey found that 60% of doctors planned to take a Covid vaccine, but only 40% of nurses intended to, Health Commissioner Judith Persichilli said in a recent “60 Minutes” segment about Operation Warp Speed.
Fauci, along with other respected public health officials and workers, should get vaccinated live on CNN. Stream it on YouTube and Twitch. It won’t convert the anti-vax, anti-mask, QAnon wingnuts (nothing will) but if you can at least get healthcare workers and at-risk folks on board, it would be time well spent.
But that’s only one small piece of the puzzle. Braswell’s piece is long and comprehensive look at the challenges regarding the Covid-19 vaccines and is worth reading all the way through.
Based on the four separate conversations I had with friends this weekend (and reading/watching assorted social media posts), it seems like everyone is really struggling with the pandemic right now, perhaps more so than back in March/April/May. Fatigue is really starting to set in, misinformation is wearing people down, there’s disease and death all around us, it’s tough to keep going towards an ill-defined finish line, and dealing with 9 straight months of grief is just not sustainable. I myself have been all right recently, thankful I’m able to do what I can to support others, but it really varies from week to week.
A year ago, before the pandemic set in, clinical psychologist Kathryn Gordon wrote a piece for Vox on how to help people that you know through a tough time. You may have seen similar advice before — e.g. How Do You Help a Grieving Friend? — but now seems like a good time for a refresher. Here’s one of Gordon’s four tips on how to help:
Ask them how they are feeling. Then, listen non-judgmentally to their response. The simple act of asking someone how they’re doing, with an open-ended question, shows that you care. Listen attentively rather than interrupting or offering your opinion. Ask simple follow-up questions like, “What does that feel like?” or “What has been on your mind as you’re going through this?” This communicates that you genuinely want to know how they’re doing and feel comfortable hearing the truth.
I hope you’re getting the support you need during all of this and are able to find small pockets of time & energy in which to be useful to those around you. ♥
My friend Jodi Ettenberg spent a decade traveling around the world, so she’s got friends and followers from all over the place. Over the weekend, she asked her Instagram followers to share their pandemic experiences and she’s been republishing them in Story collections: one, two, three. (You can also find them on her Instagram profile page.) Individually and as a collection, the stories she’s received are fascinating and heartbreaking to read. Almost 11 months into the pandemic — Wuhan’s lockdown began on Jan 23 — folks out there are really struggling and the response of governments around the world has varied widely (and wildly). Here are a few of the stories…check out the links above to read the rest.
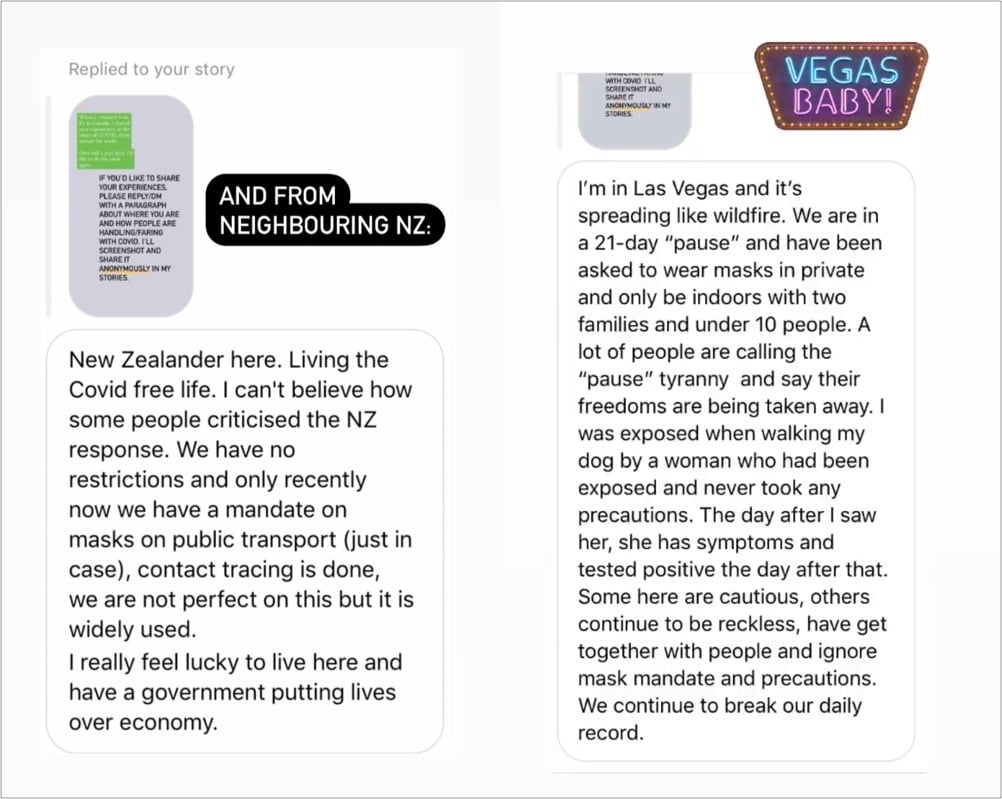
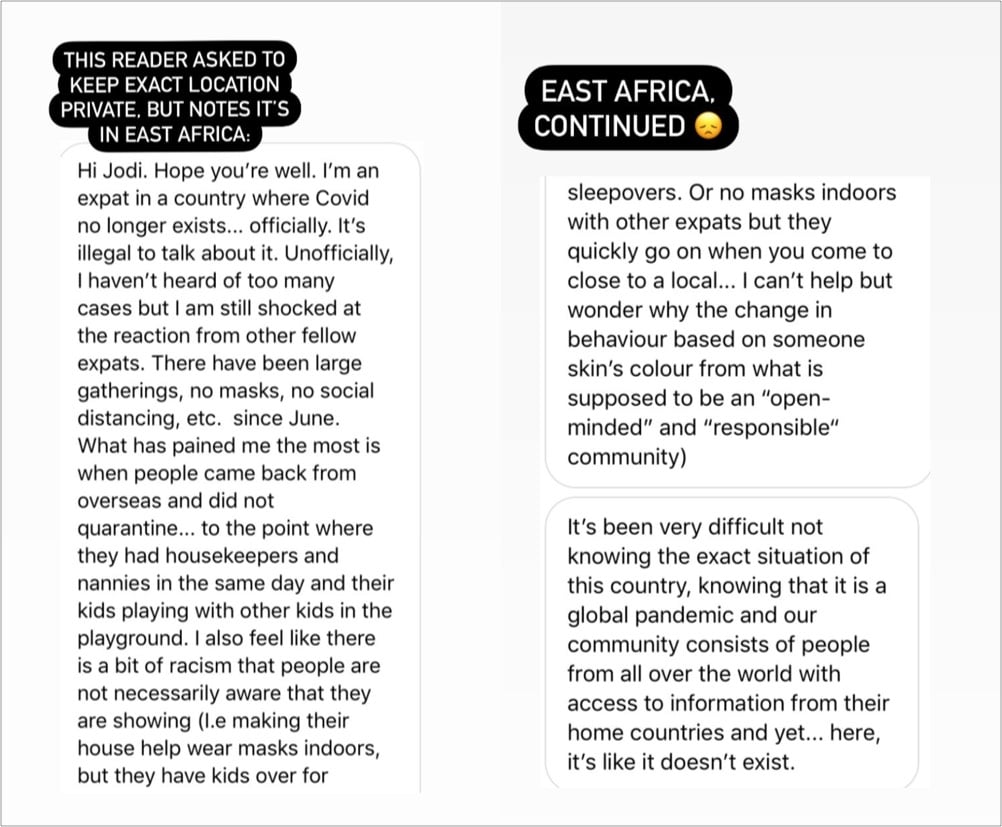
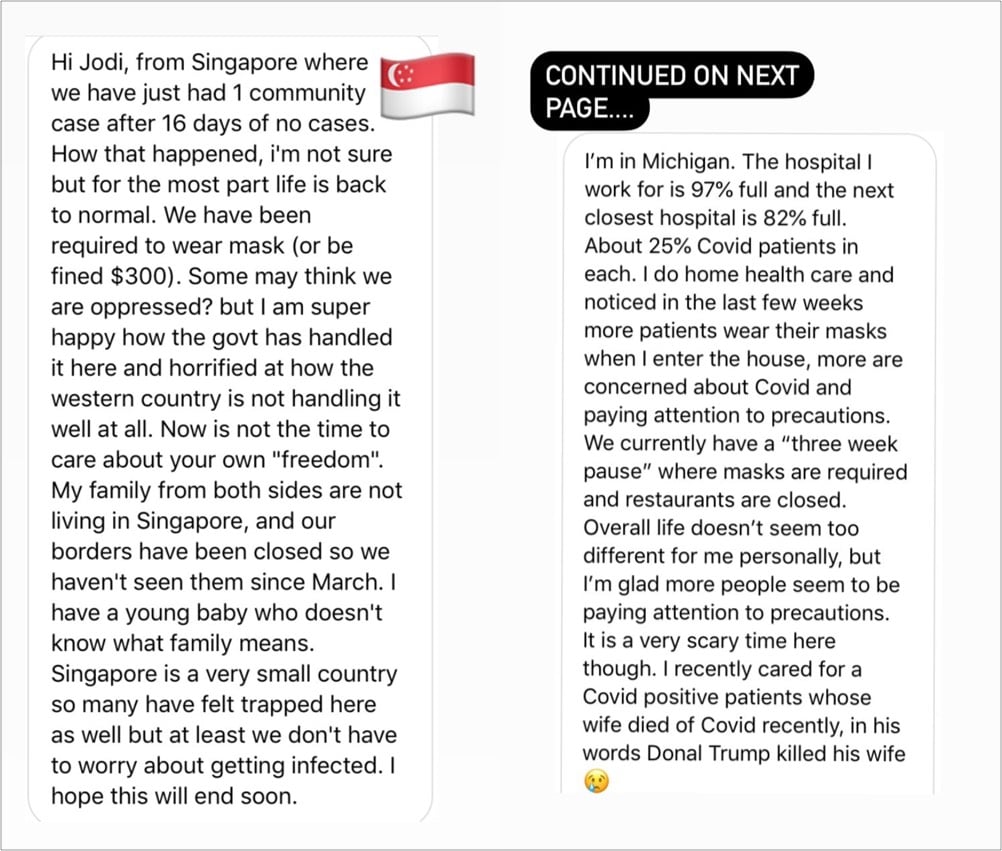
She’s still gathering & sharing stories from people, so send her a DM on Instagram about how things are going in your part of the world if you’d like to participate.
I solicited stories like this from folks back in early April. It’s surreal reading those responses now — so much completely avoidable death and suffering has occurred between then and now.
After Terri Nelson noticed people complaining online about a lack of scent from newly purchased scented candles, Kate Petrova analyzed Amazon reviews for candles from the past three years and found a drop in ratings for scented candles beginning in January 2020 (compared to a smaller ratings decline for unscented candles).
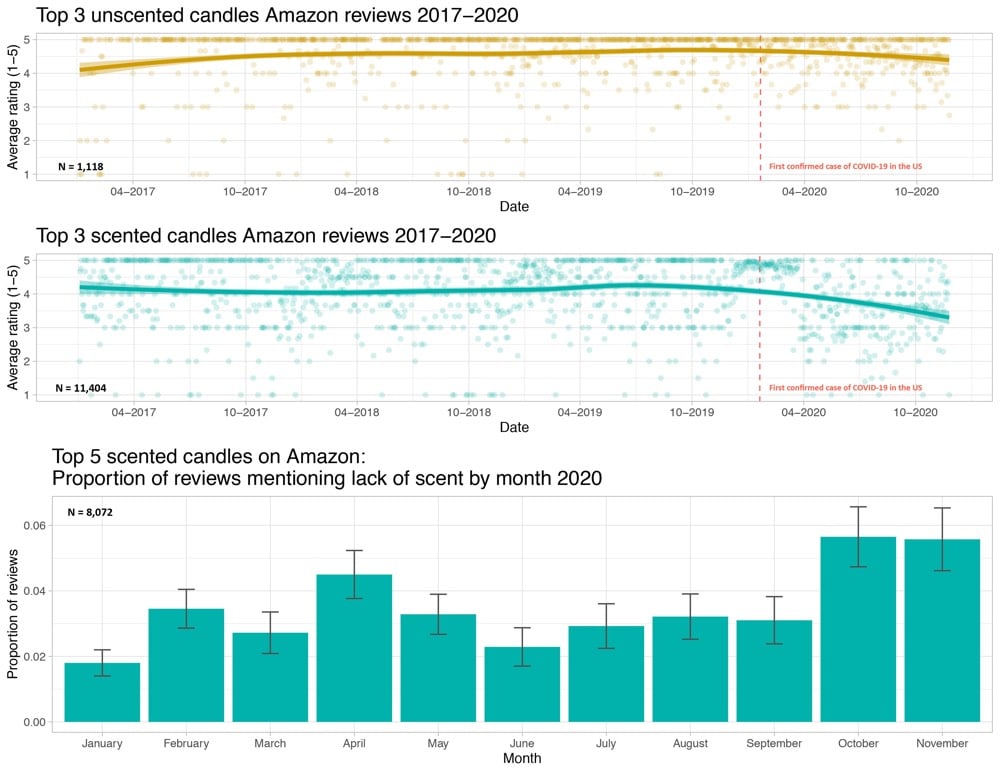
The hypothesis is that some of these buyers have lost their sense of smell due to Covid-19 infections and that’s showing up in the ratings.
With the positive news about the Covid-19 vaccine trials, I assume many of you have started to think about the potential end of the pandemic — what we’ll do, where we’ll go, who we’ll see, and reckon with what’s changed and what’s been lost. I know I have. Alex Hutchinson has written an intriguing piece on what sports science might be able to tell us about the psychology of a situation like the pandemic, where the finish line is poorly defined, ever-changing, or even non-existent.
As it happens, there’s a whole subfield of sports science, at the intersection of physiology and psychology, that explores this terrain. It’s called teleoanticipation, a term coined in 1996 by German physiologist Hans-Volkhart Ulmer to describe how our knowledge of an eventual endpoint (or telos) influences the entirety of an experience. Using endurance sports as their medium, researchers in this subfield have probed what happens when you hide the finish line, surreptitiously move it or take it away entirely. For those of us tempted by promising vaccine updates to start fantasizing about an end to the pandemic, these researchers have some advice: don’t.
Instead, the key seems to be remaining in the moment instead of focusing on the goal.
It turns out that, if you ask yourself “Can I keep going?” rather than “Can I make it to the finish?” you’re far more likely to answer in the affirmative.
This squares with mindfulness practices from Buddhism and Stoicism but also reminds me of a motivational trick I first heard a few years ago: that you can do anything for 10 seconds — and then you just begin a new 10 seconds. Turns out that was popularized by Unbreakable Kimmy Schmidt. Good advice can come from anywhere.
Even though we’re still in the midst of it, The Atlantic commissioned three designers/artists to design hypothetical Covid-19 memorials. Ian Bogost writes:
So this might seem like a strange time to imagine memorializing the pandemic in a formal way. A premature time. Maya Lin’s Vietnam Veterans Memorial was conceived in 1981, six years after the United States had withdrawn from the conflict. Michael Arad and Peter Walker’s 9/11 memorial broke ground at the site of the World Trade Center in 2006, almost five years after the attacks.
But there are downsides to waiting. A traumatic event is an author of its own memorial; as a famous anecdote attests, when a Nazi soldier asked Pablo Picasso if he had made Guernica, the famous painting the artist created during the month following the Luftwaffe’s bombing of its Basque namesake in 1937, Picasso replied, “No, you did.” The feelings, facts, and ideas available during a calamity dissipate as it ebbs. The temptation arises to contain tragedy in a tidy box, closing the book on its history.
Each of the three ideas is intriguing in its own way. I liked how Ronald Rael and Virginia San Fratello (who made those border wall teeter-totters last year) explained their thought process (which Rael elaborated on here).
Quarantine has limited our ability to use smell and touch for communion, so she and Rael became interested in finding a way to replicate the experience. That’s where pennies come in: Copper is an antiviral — a quality with obvious symbolism in the moment — and one that evolves over time, developing a patina as it interacts with water and air. So the pair latched on to it as a material.
Rael San Fratello’s first idea was a pragmatic one: a traditional memorial made of copper molded into a bulbous, organic wall. The copper material would invite the touch lost to quarantine. Outdoors, it could develop a green or purple patina. “If touched constantly,” San Fratello said, “the patina might never occur, and the memorial will remain shiny.”
See also the design for a pandemic memorial already in the planning stages in Uruguay.
Now that the preliminary results of various Covid-19 vaccine trials are coming out (and looking promising), attention is turning to the eventual distribution of the vaccines. The logistics of getting the doses out to hospitals, clinics, and doctor’s offices is one concern but so is the question of who should get vaccinated first. Supplies of the vaccines will be limited at first, so we’ll need to decide as a society what distribution method is most fair and is of the most benefit to the greatest number of people.
To this end, and in response to a request by the CDC and NIH, the National Academies of Sciences, Engineering, and Medicine formed a committee to produce a report called Framework for Equitable Allocation of COVID-19 Vaccine. The 252-page report is available to the public for free to read online or download.
In addition several recommendations — including that the vaccine be distributed to everyone free of charge — a central feature of the report is a four-phase system of vaccine distribution, summarized in this graphic:
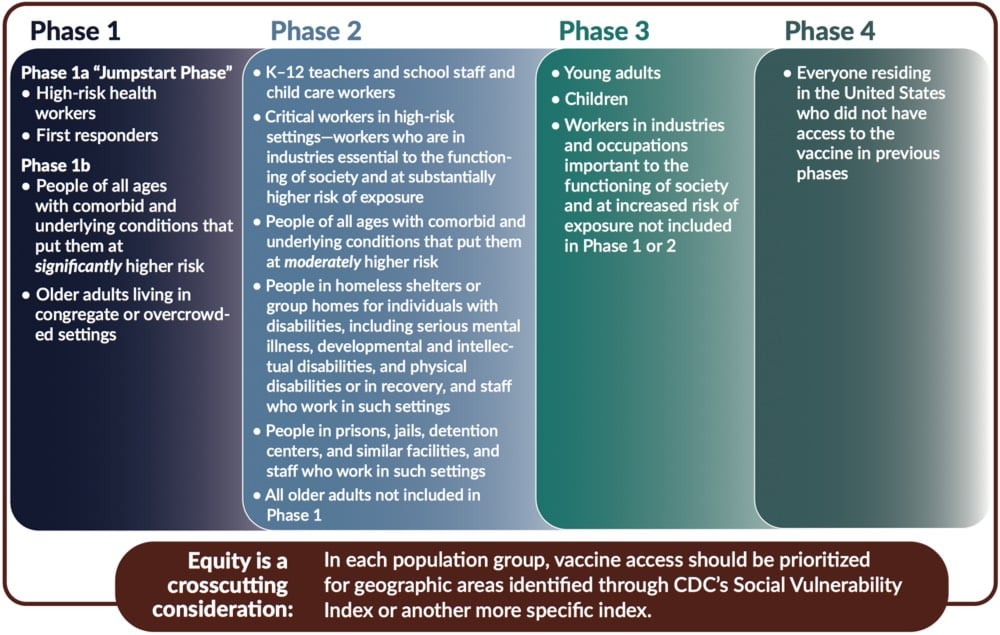
I’d like to stress that this graphic does not show all groups of people included in each phase — please consult the text of the report for that before you go sharing that graphic on social media without context. For example, here’s the full description for “high-risk health workers” in Phase 1a:
This group includes frontline health care workers (who are in hospitals, nursing homes, or providing home care) who either (1) work in situations where the risk of SARS-CoV-2 transmission is higher, or (2) are at an elevated risk of transmitting the infection to patients at higher risk of mortality and severe morbidity. These individuals — who are themselves unable to avoid exposure to the virus — play a critical role in ensuring that the health system can care for COVID-19 patients.
These groups include not only clinicians (e.g., nurses, physicians, respiratory technicians, dentists and hygienists) but also other workers in health care settings who meet the Phase 1a risk criteria (e.g., nursing assistants, environmental services staff, assisted living facility staff, long-term care facility staff, group home staff, and home caregivers). The health care settings employing these workers who are at increased risk of exposure to the virus may also include ambulatory and urgent care clinics; dialysis centers; blood, organ, and tissue donation facilities; and other non-hospital health care facilities. Finally, there are community and family settings where care for infected patients occurs. Not all the workers in these settings are paid for their labor, but, while they are caring for infected people, they all need to be protected from the virus.
Situations associated with higher risk of transmission include caring for COVID-19 patients, cleaning areas where COVID-19 patients are admitted, treated, and housed, and performing procedures with higher risk of aerosolization such as endotracheal intubation, bronchoscopy, suctioning, turning the patient to the prone position, disconnecting the patient from the ventilator, invasive dental procedures and exams, invasive specimen collection, and cardiopulmonary resuscitation. In addition, there are other frontline health care workers who, if they have uncontrolled exposure to the patients or the public in the course of their work, should be in this initial phase. This group includes those individuals distributing or administering the vaccine — especially in areas of higher community transmission — such as pharmacists, plasma and blood donation workers, public health nurses, and other public health and emergency preparedness workers. The committee also includes morticians, funeral home workers, and other death care professionals involved in handling bodies as part of this high-risk group.
The report declines to list specific industries which would be covered in Phase 2’s “critical workers in high-risk settings” but generally says:
The industries in which these critical workers are employed are essential to keeping society and the economy functioning. Since the beginning of the pandemic, millions of people have been going to work and risking exposure to the virus to ensure that markets have food; drug stores have pharmaceutical products; public safety and order are maintained; mail and packages are delivered; and buses, trains, and planes are operating.
Note also the text at the bottom of the graphic: they recommend that within each phase, priority be given to geographic areas where folks are more socially vulnerable in situations like these (e.g. as represented in the CDC’s Social Vulnerability Index).
In developing this phased approach, the committee focused on those who are at the most risk of exposure, severe illness or death, and passing along the virus to others as well as critical workers:
Risk of acquiring infection: Individuals have higher priority to the extent that they have a greater probability of being in settings where SARS-CoV-2 is circulating and of being exposed to a sufficient dose of the virus.
Risk of severe morbidity and mortality: Individuals have higher priority to the extent that they have a greater probability of severe disease or death if they acquire infection.
Risk of negative societal impact: Individuals have higher priority to the extent that societal function and other individuals’ lives and livelihood depend on them directly and would be imperiled if they fell ill.
Risk of transmitting infection to others: Individuals have higher priority to the extent that there is a higher probability of their transmitting the infection to others.
You should read (or at least skim) the full report for more information about the plan and the rationale behind it.
On a personal parting note, as someone who is squarely in the 5-15% of Americans covered in Phase 4 — more specifically: as a 40-something straight white man who non-essentially works from home, isn’t low-income, doesn’t socialize widely even under normal circumstances, and should probably be the very last person on this whole Earth scheduled to be vaccinated under an equitable framework — I am content to wait my turn should the US adopt this framework or something like it.1 Distributing vaccines to those who need them most is absolutely the right thing to do, both ethically and from the standpoint of getting society “back to normal” as quickly as possible and with as little additional death and suffering as possible.
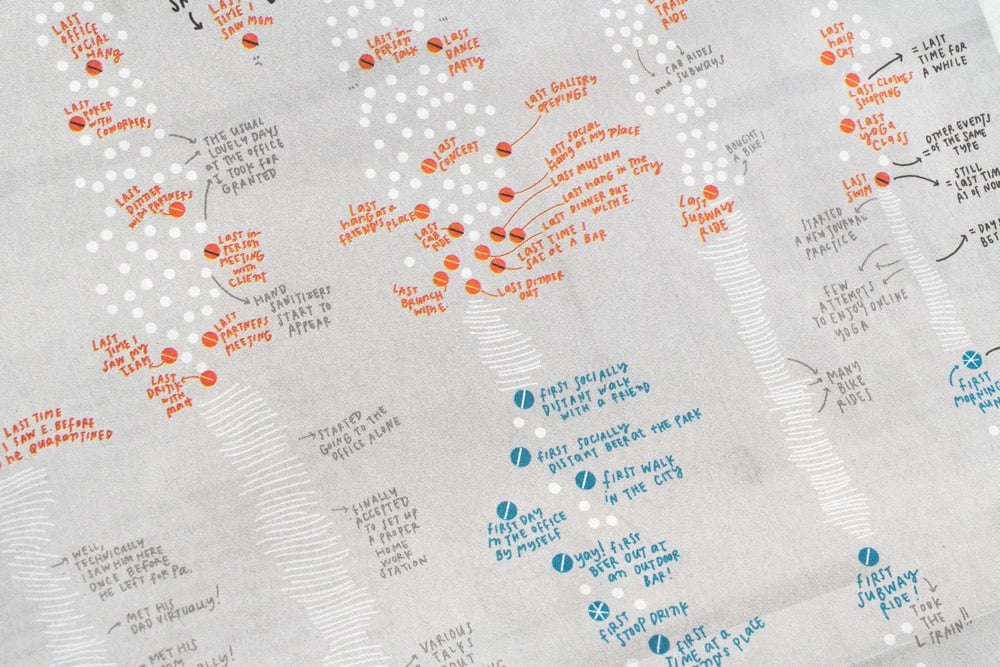
For the print version of the NY Times from this past Sunday, information designer Giorgia Lupi created a hand-drawn visualization that “tracks the last time [she] did something before the pandemic hit, and the first time she did something new with social distancing”.
Our lives have been transformed during the Covid-19 pandemic as the activities we used to do every day have been put on hold and new, socially distanced routines have taken their place. Pentagram partner Giorgia Lupi documents these changes in her own life in a data visualization commissioned by The New York Times for the cover of its “At Home” section, which runs as part of the newspaper’s Sunday edition. The hand-drawn visualization is a personal timeline that tracks the “last” time Giorgia did something before the pandemic hit, and the “first” time she did something new as she started to emerge from lockdown.
Not hand-drawn, but I remember pretty clearly what my lasts were:
- Last movie (w/ kids): Onward in mid-March
- Last movie (solo): Portrait of a Lady on Fire in mid-March
- Last visit to NYC: late October 2019
- Last trip: Vietnam/Singapore/Qatar in Jan/Feb 2020
- Last restaurant (solo): a forgettable ramen place in Burlington in mid-March
- Last restaurant (w/ a friend): better local ramen place in early March
- Last cocktail bar: Bar Stories in Singapore in early February
- Last museum: Museum of Islamic Art in Doha, Qatar in early February
I don’t remember my firsts as well, although one that sticks out is eating french fries (take-out) in July. On a normal day, french fries are delicious but when you haven’t had them in months, they are otherworldly.
Preliminary results from the trials of the Covid-19 vaccine jointly developed by the University of Oxford and AstraZeneca indicate that the vaccine’s overall efficacy is 70% but that a regimen that calls for a lower first dose is 90% effective.
The preliminary results on the AstraZeneca vaccine were based on a total of 131 Covid-19 cases in a study involving 11,363 participants. The findings were perplexing. Two full doses of the vaccine appeared to be only 62% effective at preventing disease, while a half dose, followed by a full dose, was about 90% effective. That latter analysis was conducted on a small subset of the study participants, only 2,741.
Hopefully more study will be done on that dosage question. From the AP:
“The report that an initial half-dose is better than a full dose seems counterintuitive for those of us thinking of vaccines as normal drugs: With drugs, we expect that higher doses have bigger effects, and more side-effects,” he said. “But the immune system does not work like that.”
The seemingly lower efficacy comes with some perhaps significant benefits: this vaccine is cheaper to produce and doesn’t require any special refrigeration.
The vaccine can be transported under “normal refrigerated conditions” of 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit), AstraZeneca said. By comparison, Pfizer plans to distribute its vaccine using specially designed “thermal shippers” that use dry ice to maintain temperatures of minus-70 degrees Celsius (minus-94 degrees Fahrenheit).
The Pfizer and Moderna vaccines were pretty similar in many respects and this one seems quite different. These results were just released a few hours ago, so it will be interesting to follow the debate and expert commentary on this. Stay tuned…
Update: This is amazing: the seemingly more effective 1/2 dose + full dose regimen was a mistake.
Around the time when Astra was initiating its partnership with Oxford at the end of April, university researchers were administering doses to trial participants in Britain.
They soon noticed expected side effects such as fatigue, headaches or arm aches were milder than expected, he said.
“So we went back and checked … and we found out that they had underpredicted the dose of the vaccine by half,” said Pangalos.
A far smaller number of participants was given the initial half-dose, so more research will need to be done to determine if this mistake will be added to the long list of scientific discoveries made because of errors. There’s a good piece in Nature that talks about what we know and don’t know about the vaccine results so far along with some informed speculation.
But, if the differences are bona fide, researchers are eager to understand why. “I don’t think it’s an anomaly,” says Katie Ewer, an immunologist at Oxford’s Jenner Institute who is working on the vaccine. “I’m keen to get into the lab and start thinking about how we address that question.” She has two leading theories for why a lower first dose might have led to better protection against COVID. It’s possible that lower doses of vaccine do a better job at stimulating the subset of immune cells called T cells that support the production of antibodies, she says.
Another potential explanation is the immune system’s response against the chimpanzee virus. The vaccine triggers an immune response not only to the SARS-CoV-2 spike protein, but also to components of the viral vector. It’s possible that the full first dose blunted this reaction, says Ewer. She plans to look at antibody responses against the chimpanzee virus to help address this question.
Update: A short thread by Dr. Natalie Dean, which leads with “AstraZeneca/Oxford get a poor grade for transparency and rigor when it comes to the vaccine trial results they have reported”.
COVID-19 has required all of us to scrutinize our actions and sacrifice our desires and even our obligations in order to keep ourselves and those around us safe. I want to examine two cases where reasonable, well-informed, and influential people make entirely different choices based on largely similar evidence.
You may have heard that MSNBC host Rachel Maddow has been quarantining at home following close contact with a person who had tested positive for COVID-19. You may have also heard that last night, Maddow returned to her show (still filming from home) to reveal that this person was her partner of 20+ years, artist/photographer Susan Mikula. Mikula is recovering, but at at least one point, the couple genuinely feared for her life. Maddow herself is still testing negative; with Mikula in much less danger and Maddow nearing the end of quarantine, they felt it was time to open the curtain on their experience.
If you haven’t seen it already, I’d like you to watch the video of Maddow describing her experience of living with a loved one who is suffering from COVID-19, whom you have to care for but cannot touch without grave risk to yourself, and then to others. (It is about Mikula’s own experience, but it’s really much more about Maddow’s experience, for good reason.)
Here’s a quick excerpt, if you want a textual preview (via Vulture):
“Just believe me: Whatever you have calculated into your life as acceptable risk, as inevitable risk, something that you’re willing to go through in terms of this virus because statistically, hey probably, it will be fine for you and your loved ones, I’m just here to tell you to recalibrate that,” [Maddow] warned. “Frankly, the country needs you to recalibrate that because broadly speaking, there’s no room for you in the hospital right now.”
She cites hospitals being overwhelmed with a “50 percent” increase in patients “in two weeks.” While it may be easy to risk your own life, the virus doesn’t let you make the choice. “What you need to know is whoever’s the most important person in your life, whoever you most love and most care for and most cherish in the world, that’s the person who you may lose and who you may spend weeks up all night freaking out about and calling doctors all over the place and over and over again all night long, trying to figure out how to keep that person breathing and out of the hospital,” she said. “Whatever you’re doing, however you’ve calibrated risk in your life, don’t get this thing.”
Another moment worth noting in the video is shortly after she begins. Maddow is interrupted by a recurring beeping noise in a room off-camera. She has to attend to it herself, in the middle of a live television show, because there’s no one else at home who can do it. She takes off her microphone and earpiece, then has to put it back on. After already revealing at the beginning of the show that she’s not wearing makeup—she doesn’t know how to apply it herself, and no one can help her—it’s a nice peek behind the scenes.
I don’t know if everyone always understands how much work it takes it is to perform for live television: how many accessories you need, how much support is required. People don’t see what you have to look like, sound like, or act like; they don’t see the almost cyborg contraption you have to become in order to make a successful television appearance. Being good at television is a specific skill. It’s as different from writing, reporting, or public speaking as football, baseball, and basketball are from playing polo. It doesn’t matter if you have your words on a teleprompter (although that does help): you still have to deliver them, in time, no backsies, and look and sound good while you’re doing it.
The disruption of the show also happens in the middle of a charming metaphor Maddow uses to describe her relationship:
The way that I think about it is not that she is the sun and I’m a planet that orbits her—that would give too much credit to the other planets. I think of it more as a pitiful thing: that she is the planet and I am a satellite, and I’m up there sort of beep-beep-beeping at her and blinking my lights and just trying to make her happy.
Compare this to Farhad Manjoo’s essay in The New York Times today, “I Traced My COVID-19 Bubble and It’s Enormous.” Manjoo starts with a classic dilemma: he knows it’s unsafe in general to travel for Thanksgiving, but he wonders if it might be safer for his family, given the size of their social circle and the precautions they’ve taken. He’d like to find out more, to replace his general intuitions, which pull him in both directions, with something more concrete. This is a time-honored journalistic premise (a rhetorical trope, really) for answering a question many people might have.
In researching his close contacts, and their own exposure to other people, Manjoo quickly has cold water thrown on the notion that his bubble is in any way contained to the degree he’d imagined it to be. (This part of the story is well-illustrated: I’ll give you the text excerpts, but it’s worth clicking through and scrolling through yourself.)
I thought my bubble was pretty small, but it turned out to be far larger than I’d guessed.
My only close contacts each week are my wife and kids.
My kids, on the other hand, are in a learning pod with seven other children and my daughter attends a weekly gymnastics class.
I emailed the parents of my kids’ friends and classmates, as well as their teachers, and asked how large each family’s bubble was.
Already, my network was up to almost 40 people.
Turns out a few of the families in our learning pod have children in day care or preschool.
And one’s classmate’s mother is a doctor who comes into contact with about 10 patients each week.
Once I had counted everyone, I realized that visiting my parents for Thanksgiving would be like asking them to sit down to dinner with more than 100 people.
He isn’t actually done counting yet: from himself, he’s only gone to three degrees of separation. But presumably, the point in the headline is made. The author’s bubble is enormous, and presumably the reader’s is, too.
Then a curious thing happens. Manjoo decides that what he’s learned doesn’t matter. He thinks his family and his contacts are special after all. “All of my indirect contacts are taking the virus seriously—none of them spun conspiracy theories about the pandemic, or suggested it was no big deal or told me to bug off and mind my own business.” (This is a very low threshold for “taking the virus seriously.”) And he would really like to take his wife and children to see his parents. An epidemiologist gives him some cover, saying his desire to see their parents is understandable, and it’s all a matter of assessing and evaluating risk.
So, he changes his mind again. He makes a few concessions (drive, not fly; an outdoor meal rather than an indoor one; staying off-site rather than sleeping over). And he’s going to travel five hours each way with his wife and children and their 100+ direct and indirect contacts to celebrate Thanksgiving with his parents.
This is contrarianism on a scale not usually seen in a newspaper article. (They’re usually too short to take this many turns.) It is one thing to counter received wisdom by posing a counterfactual. It is another to spend hours of reporting, gathering facts, calling in experts, putting everything on the record, and then deciding that none of that matters.
On Twitter, I called it “the full Gladwell”; only Malcolm Gladwell at The New Yorker can consistently pull this hairpin twist off and stick the landing, even if he frequently violates good sense and plain facts to do it.
It’s important, though, that this is not just a rhetorical trick. These are the real lives of real people, both in the story itself, and radiating out to its readers and their contacts in a global newspaper, the United States’ paper of record. And the reasoning and evidence that are considered but discarded gives the illusion that this is a choice motivated not by setting reason aside, but considering all options and maximizing one’s expected utility.
Not to “both sides” this, but I’m gonna “both sides” this: in some sense, both Maddow and Manjoo are putting their thumb on the scales, in opposite directions. For Maddow, the experience of almost losing the love of her life makes it so that she would take no willing risk that might endanger her or anyone else. (She acknowledges that a certain amount of unavoidable, unwilling risk remains.)
Manjoo is different. He acknowledges that he has no such experience. He is less concerned with the possible loss of his parents’ lives than the loss of their presence in his life and in their childrens’ lives. He sees the willing assumption of risk as an open moral question, and something that can be calculated and appropriately mitigated.
Maddow has constructed a universe where she is a tiny satellite orbiting a much larger planet, whose continued health and existence is the central focus of her concern. Manjoo has drawn a map with himself at its center, where anyone beyond the reach of his telephone falls off the edges.
Maddow is also explicitly pleading with her viewers to learn what they can from her experience, and adjust their behavior accordingly. Manjoo is performing his calculus only for himself; he implicitly presents himself as a representative example (while also claiming he and his circle are extraordinarily conscientious and effective), but each reader can draw their own conclusions and make their own decision.
At this point the balancing dominoes tip over. Maddow’s position, her argument, and her example are clearly more moral and more persuasive than Manjoo’s. Manjoo’s essay is worth reading, but the conclusion is untenable. It doesn’t do the work needed to arrive there or persuade anyone else to do the same. And at a time when many people are spinning conspiracies about the pandemic, or claiming that it’s no big deal, and in turn influencing others—when we haven’t even yet considered the virus’s impact on the uncounted number of people, from medical staff and many other essential workers to prisoners and the impoverished, who do not simply get to choose how to spend their holiday—it’s irresponsible.
The larger moral tragedy is that because our leaders have failed, and too often actually worked to damage the infrastructure, expertise, and goodwill accumulated over generations, we have no consistent, authoritative guidance on what we should and should not do. We do not know who to trust. We have no money, no help, and no plan but to wait. We have no sense of what rules our friends and neighbors, colleagues and workers, are following when they’re not in our sight; we don’t even know what practices they would even admit to embracing. We have no money; we have no help. We are left on our own, adrift in deep space, scribbling maps and adding sums on the back of a napkin. We are all in this together, yet we are completely alone.
For Vox, Julia Belluz takes a look at the approach that’s made Vermont more successful than most other US states in combatting Covid-19. The big thing? State officials recognized that those most at risk needed more support.
There’s a fatal flaw embedded in the basic Covid-19 test, trace, and isolate trifecta used around the world: It doesn’t account for the fact that the coronavirus is not an equal-opportunity pathogen. The people who are most likely to be tested, and to have the easiest time quarantining or isolating, are also the least likely to get sick and die from the virus.
From the United Kingdom to Sweden to Canada, we have evidence that the virus preys on people employed in “essential service” jobs (bus drivers, nurses, factory workers), which don’t allow for telecommuting or paid sick leave; people in low-income neighborhoods; and people in “congregate housing” like shelters, prisons, and retirement homes.
People of color tend to be overrepresented in these groups — but there’s no biological reason they’re more likely to get sick and die from the virus. Simply put: They tend to work jobs that bring them outside the home and into close contact with other people, live in crowded environments ideal for coronavirus contagion, or both.
The state then directed efforts, resources, and money to nursing homes, the unhoused, prisons, and essential workers to make it easier for those folks to stay safe.
I also thought this bit was really interesting:
There’s a simple adage in public health: “Never do a test without offering something in exchange,” said Johns Hopkins’s Stefan Baral. So when a patient gets tested for HIV, for example, they’re offered treatment, support, or contact tracing. “We’re not just doing the testing to get information but also providing a clear service,” Baral added, and potentially preventing that person from spreading the virus any further. “This is basic public health.”
With Covid-19, the US has failed at basic public health. Across the country, people have been asked to get tested without anything offered in exchange.
“If we are asking people to stay home and not work, we have to make sure society is supporting them,” Baral said. “An equitable program would support people to do the right thing.”
“Never do a test without offering something in exchange.” To the extent that federal and state governments have been asking to people to stay home, get tested, and wear a mask, many of those same governments have been unwilling or unable to provide people with much in return for doing so. And so, here we are months into this, paying for that inaction with 250,000 lives.
Update: How NYC does “never do a test without offering something in exchange”:
You can access a free hotel room to safely isolate from your family, which include meals, Rx delivery, free wi-fi, medical staff on site, and transportation to and from hotel and medical appointments.
(via @agoX)
As I write this, it’s snowing outside here in Vermont and Covid-19 has finally gained a foothold in our little state. At the governor’s press conference yesterday, he and his pandemic response team announced that contact tracing done by the state showed that the rise in cases started as an outbreak in some hockey leagues. That initial outbreak wasn’t contained and subsequent non-essential, indoor, mask-less, multi-household gatherings and Halloween parties resulted in the very sharp rise we started to see here in the first week of November.
Scott explained that 71% of outbreaks reported from Oct. 1 to Nov. 13 were linked to “social events, parties and people hanging out at home or bars and clubs.” He added Vermont has not seen the virus spread widely at schools, restaurants or other businesses.
Dr. Mark Levine, the state health commissioner, said those parties came in a variety of sizes of parties — Halloween gatherings large and small, dinner parties, baby showers, “people in the high single numbers at a deer camp.”
In states with many infections, particularly in the Midwest, contact tracing is all but impossible, so it’s instructive to pay attention to Vermont’s example here: we’re doing the tracing and the tracers say the infections are coming from people gathering indoors across multiple households. Which is exactly what public health and medical experts have been urging people not to do for months now.
And that brings us to Thanksgiving. For The Atlantic, Rachel Gutman asked her colleagues who have been writing extensively about the pandemic for some of their top safety rules and guidelines and their number one was, say it with me:
My colleagues’ guidance boils down to this winter’s golden rule for interacting with anyone outside your immediate household: Don’t spend time indoors with other people.
Here it is again in a fun font, just to make sure you got it: 𝓓𝓸𝓷’𝓽 𝓼𝓹𝓮𝓷𝓭 𝓽𝓲𝓶𝓮 𝓲𝓷𝓭𝓸𝓸𝓻𝓼 𝔀𝓲𝓽𝓱 𝓸𝓽𝓱𝓮𝓻 𝓹𝓮𝓸𝓹𝓵𝓮.
Look, for some people spending time indoors with others is essential — jobs, education, etc. — but those who don’t have to, shouldn’t. And this goes for everywhere in the US because no states (aside from maybe Hawaii) are doing well right now — cases are either high, rising sharply, or both. Please please don’t gather in indoor, multi-household groups for Thanksgiving if you haven’t quarantined beforehand. In the US right now, about 1-in-55 people who get Covid-19 die from it. With rates already high around the country, if many people do Thanksgiving as usual, an already horrific and deadly situation could become much much worse.
According to an unpublicized report by the Chinese government, the first documented case of Covid-19 was a 55-year-old person living in Hubei province on November 17, 2019. That makes today the first anniversary of the start of the Covid-19 pandemic. From that person (and possibly earlier or concurrent cases), the disease slowly and silently spread until it was determined to be due to a novel coronavirus.
They found that following the Nov. 17 case, about one to five new cases were reported every day and by Dec. 15, the total infections reached 27. Daily cases seem to have increased after that, with the case count reaching 60 by Dec. 20, the SCMP reported.
On Dec. 27, Dr. Zhang Jixian, head of the respiratory department at Hubei Provincial Hospital, reported to health officials in China that a novel coronavirus was causing the disease; by that day, it had infected more than 180 individuals. (Doctors may not have been aware of all of those cases at the time, but only identified those cases after going back over the records, the Morning Post reported.)
No one had any idea how much the world was going to change that day. What an awful, humbling, terrifying, ghoulish year.
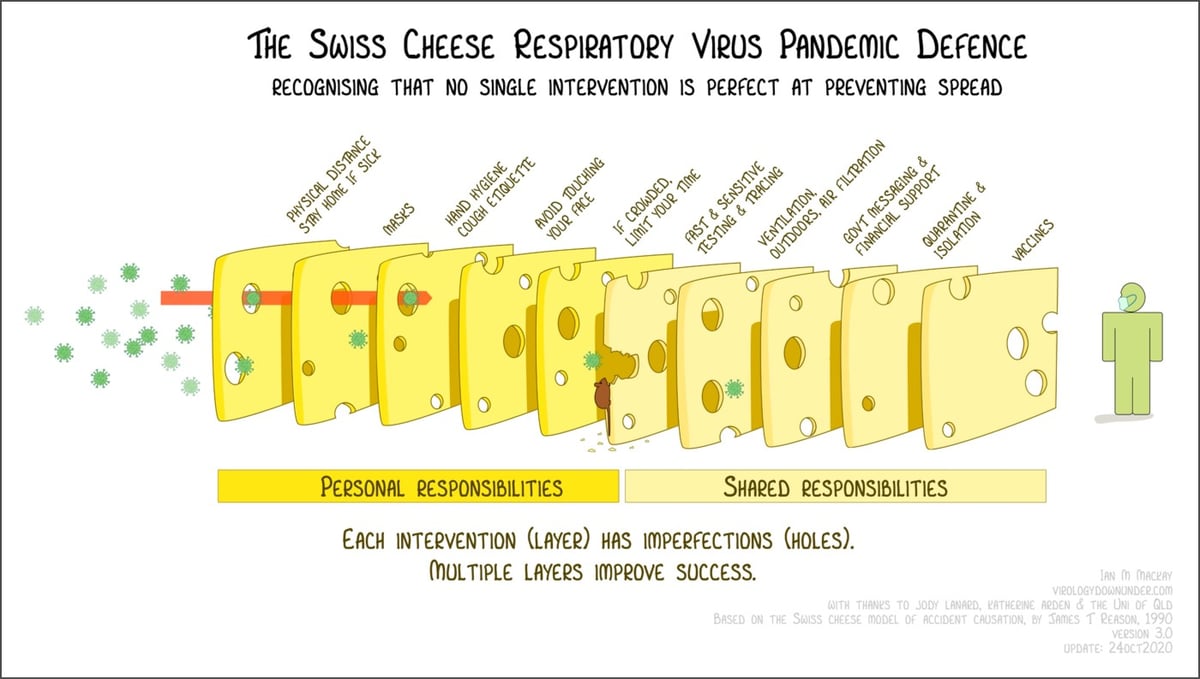
The Swiss cheese model of accident causation is a framework for thinking about how to layer security measures to minimize risk and prevent failure. The idea is that when several layers of interventions, despite their weaknesses, are properly stacked up between a hazard and a potentially bad outcome, they are able to cumulatively prevent that outcome because there’s no single point of failure. During the pandemic, health care workers and public health officials have been using the Swiss cheese model to visualize how various measures can work together to help keep people safe.
Virologist Dr. Ian Mackay has visualized the Swiss cheese Covid-19 defense in a wonderful way (pictured above). Each layer of cheese represents a personal or shared intervention — like mask wearing, limiting your time indoors w/ crowds, proper ventilation, quarantine, vaccines — and the holes are imperfections. Applied together, these imperfect measures work like a filter and can vastly improve chances of success.1 He even added a “misinformation mouse” chewing through one of the cheese slices to represent how deceptive information can weaken these defenses.
Mackay has released this graphic under a Creative Commons license (free to share and adapt w/ attribution) and is available in English, German, French, Spanish, Korean, and several other languages. (via @EricTopol)
Zeynep Tufekci says that a devastating third pandemic surge is upon us and that It’s Time to Hunker Down. She leads with the good news (vaccines, treatments, knowledge, testing capacity & quickness) but notes that with winter coming and a high baseline of cases from a summer not spent in preparation, now is the time to really knuckle down so that we can get to the finish line.
Whatever the causes, public-health experts knew a fall and winter wave was a high likelihood, and urged us to get ready.
But we did not.
The best way to prepare would have been to enter this phase with as few cases as possible. In exponential processes like epidemics, the baseline matters a great deal. Once the numbers are this large, it’s very easy for them to get much larger, very quickly — and they will. When we start with half a million confirmed cases a week, as we had in mid-October, it’s like a runaway train. Only a few weeks later, we are already at about 1 million cases a week, with no sign of slowing down.
Americans are reporting higher numbers of contacts compared with the spring, probably because of quarantine fatigue and confusing guidance. It’s hard to keep up a restricted life. But what we’re facing now isn’t forever.
It’s time to buckle up and lock ourselves down again, and to do so with fresh vigilance. Remember: We are barely nine or 10 months into this pandemic, and we have not experienced a full-blown fall or winter season. Everything that we may have done somewhat cautiously — and gotten away with — in summer may carry a higher risk now, because the conditions are different and the case baseline is much higher.
Newer posts
Older posts
Socials & More