kottke.org posts about medicine
The development of vaccines against infectious diseases is among the greatest of human accomplishments and has saved ten of millions of people from dying. And yet some are still hung up on their side effects (and also the widely disproved and debunked fraudulent claim that vaccines cause autism). In this video, Kurzgesagt looks at how vaccines work and compares the impact of their side effects (minuscule) to the potential effect of the diseases they protect against (children dying).
The extensive list of sources they used for the video can be found here.
The title of this video is “The Side Effects of Vaccines - How High is the Risk?”, which seems like it’s maximized for clicks and to spread amongst anti-vaxxers on social media. I wish it had a more accurate title — something like “The Absurdly Low Risk of Vaccine Side Effects” or maybe “Vaccines. And Now My Kids Don’t Die.” — but perhaps positioning it this way is a good strategy to get folks who may not be quite so radicalized to watch it.
In her new book, Invisible Women: Data Bias in a World Designed for Men, Caroline Criado Perez argues that the data that scientists, economists, public policy makers, and healthcare providers rely on is skewed, unfairly and dangerously, towards men.
…because so much data fails to take into account gender, because it treats men as the default and women as atypical, bias and discrimination are baked into our systems. And women pay tremendous costs for this bias, in time, money, and often with their lives.
The Guardian has a lengthy excerpt of the book, including a discussion of crash test dummies:
Crash-test dummies were first introduced in the 1950s, and for decades they were based around the 50th-percentile male. The most commonly used dummy is 1.77m tall and weighs 76kg (significantly taller and heavier than an average woman); the dummy also has male muscle-mass proportions and a male spinal column. In the early 1980s, researchers based at Michigan University argued for the inclusion of a 50th-percentile female in regulatory tests, but this advice was ignored by manufacturers and regulators. It wasn’t until 2011 that the US started using a female crash-test dummy — although, as we’ll see, just how “female” these dummies are is questionable.
Designing cars around the typical male body type means women are more likely to be injured or killed:
Men are more likely than women to be involved in a car crash, which means they dominate the numbers of those seriously injured in them. But when a woman is involved in a car crash, she is 47% more likely to be seriously injured, and 71% more likely to be moderately injured, even when researchers control for factors such as height, weight, seatbelt usage, and crash intensity. She is also 17% more likely to die. And it’s all to do with how the car is designed — and for whom.
Another example Criado Perez cites involves women’s healthcare:
When Viagra — sildenafil citrate — was tested initially as heart medication, its well-known properties for men were discovered. “Hallelujah,” said Big Pharma, and research ceased. However, in subsequent tests the same drug was found to offer total relief for serious period pain over four hours. This didn’t impress the male review panel, who refused further funding, remarking that cramps were not a public health priority.
In this piece for The Guardian, Matthew Walker says that sleeping well is the best thing you can do for your health. Here are just a couple of examples:
Routinely sleeping less than six hours a night also compromises your immune system, significantly increasing your risk of cancer. So much so, that recently the World Health Organization classified any form of night-time shiftwork as a probable carcinogen.
Inadequate sleep — even moderate reductions of two to three hours for just one week — disrupts blood sugar levels so profoundly that you would be classified as pre-diabetic. Short sleeping increases the likelihood of your coronary arteries becoming blocked and brittle, setting you on a path towards cardiovascular disease, stroke and congestive heart failure.
A lack of sleep may also increase your chances of developing Alzheimer’s disease, decrease your athletic performance, make it more difficult to control your appetite, and have mental health consequences. Walker, who is the director of UC Berkeley’s Center for Human Sleep Science and author of Why We Sleep: Unlocking the Power of Sleep and Dreams, says we should change our cultural attitudes towards sleep.
I believe it is therefore time for us, as individuals and as nations, to reclaim our right to a full night of sleep, without embarrassment or the terrible stigma of laziness. I fully understand that this prescription of which I write requires a shift in our cultural, professional, and global appreciation of sleep.
In my media diet roundup post for 2018, I said that getting adequate sleep has “transformed my life” and that sleep is “even lower-hanging self-help fruit than yoga or meditation”. I have not been sleeping well for the past several weeks and it’s taking a toll: I’ve been sluggish, eating poorly & erratically, feeling down, and not anywhere near my peak mental performance. This morning I woke up at 4am, couldn’t really get back to sleep, and I feel like I’m running at 60% capacity, 65% tops.
Roald Dahl’s oldest daughter Olivia died from the measles when she was seven years old. She died because there wasn’t a reliable measles vaccine then, and in this heartfelt letter he wrote years later, Dahl wants everyone to know that there is such a vaccine now.
Olivia, my eldest daughter, caught measles when she was seven years old. As the illness took its usual course I can remember reading to her often in bed and not feeling particularly alarmed about it. Then one morning, when she was well on the road to recovery, I was sitting on her bed showing her how to fashion little animals out of coloured pipe-cleaners, and when it came to her turn to make one herself, I noticed that her fingers and her mind were not working together and she couldn’t do anything.
‘Are you feeling all right?’ I asked her.
‘I feel all sleepy,’ she said.
In an hour, she was unconscious. In twelve hours she was dead.
The measles had turned into a terrible thing called measles encephalitis and there was nothing the doctors could do to save her. That was twenty-four years ago in 1962, but even now, if a child with measles happens to develop the same deadly reaction from measles as Olivia did, there would still be nothing the doctors could do to help her.
On the other hand, there is today something that parents can do to make sure that this sort of tragedy does not happen to a child of theirs. They can insist that their child is immunised against measles. I was unable to do that for Olivia in 1962 because in those days a reliable measles vaccine had not been discovered. Today a good and safe vaccine is available to every family and all you have to do is to ask your doctor to administer it.
I feel so tired when I think about parents not vaccinating their children against easily preventable fatal diseases. It’s child abuse and the kids know better! Here’s a tweet from Erin Faulk sharing some screenshots of teens asking how they can get vaccinated over their parents’ objections.
“Vaccines. And now my kids don’t die.”
When Sonia Vallabh lost her mother to a rare disease called fatal familial insomnia, she soon found out that she had inherited the disease, that there was no cure, and that she’d be dead in “a decade or two”. Despite almost no scientific training, Vallabh and her husband both quit their jobs to work on a cure. Talk about going all-in.
Within a few weeks of the diagnosis, Sonia had quit her job to study science full time, continuing classes at MIT during the day and enrolling in a night class in biology at Harvard’s extension school. The pair lived off savings and Eric’s salary. Sonia had expected to take a temporary sabbatical from her real life, but soon textbooks and academic articles weren’t enough. “The practice of science and the classroom version of science are such different animals,” Sonia says. She wanted to try her hand in the lab. She found a position as a technician with a research group focusing on Huntington’s disease. Eric, not wanting to be left behind, quit his job too and offered his data-crunching expertise to a genetics lab. The deeper they dove into science, the more they began to fixate on finding a cure.
They’re now on the brink of getting their Harvard PhDs and are pushing ahead with a promising medical therapy.
As soon as the couple began their presentation, Lander says, there was a sense of “pushing on an open door” — quite a surprise, given the agency’s stodgy reputation. “People still flat-out don’t believe the FDA was cool with it,” Minikel says. Afterward, one of the 25 scientists in the audience pulled Lander aside and said, “That was one of the best presentations I’ve ever seen.” Schreiber agreed. He alluded to a pharmaceutical company he’d helped set up early in his career. “Twenty-four years into that company, there was nothing to show for it. Not one thing,” he says. “For two graduate students who are not trained in science to come in and do what they did? Absolute forces of nature, savants. They keep seeing things that other people don’t see.”
Update: D.T. Max wrote a book on prions and prion-based diseases called The Family That Couldn’t Sleep. I looked in the kottke.org archives and found a 2010 post on a National Geographic article Max wrote about sleep that specifically referenced fatal familial insomnia:
The main symptom of FFI, as the disease is often called, is the inability to sleep. First the ability to nap disappears, then the ability to get a full night’s sleep, until the patient cannot sleep at all. The syndrome usually strikes when the sufferer is in his or her 50s, ordinarily lasts about a year, and, as the name indicates, always ends in death.
(via @mattbucher)
For Outside magazine, Rowan Jacobsen talks to scientists whose research suggests that the current guidelines for protecting human skin from exposure to the sun are backwards. Despite the skin cancer risk, we should be getting more sun, not less.
When I spoke with Weller, I made the mistake of characterizing this notion as counterintuitive. “It’s entirely intuitive,” he responded. “Homo sapiens have been around for 200,000 years. Until the industrial revolution, we lived outside. How did we get through the Neolithic Era without sunscreen? Actually, perfectly well. What’s counterintuitive is that dermatologists run around saying, ‘Don’t go outside, you might die.’”
When you spend much of your day treating patients with terrible melanomas, it’s natural to focus on preventing them, but you need to keep the big picture in mind. Orthopedic surgeons, after all, don’t advise their patients to avoid exercise in order to reduce the risk of knee injuries.
Meanwhile, that big picture just keeps getting more interesting. Vitamin D now looks like the tip of the solar iceberg. Sunlight triggers the release of a number of other important compounds in the body, not only nitric oxide but also serotonin and endorphins. It reduces the risk of prostate, breast, colorectal, and pancreatic cancers. It improves circadian rhythms. It reduces inflammation and dampens autoimmune responses. It improves virtually every mental condition you can think of. And it’s free.
These seem like benefits everyone should be able to take advantage of. But not all people process sunlight the same way. And the current U.S. sun-exposure guidelines were written for the whitest people on earth.
Exposure and sunscreen recommendations for people with dark skin may be particularly misleading.
People of color rarely get melanoma. The rate is 26 per 100,000 in Caucasians, 5 per 100,000 in Hispanics, and 1 per 100,000 in African Americans. On the rare occasion when African Americans do get melanoma, it’s particularly lethal — but it’s mostly a kind that occurs on the palms, soles, or under the nails and is not caused by sun exposure.
At the same time, African Americans suffer high rates of diabetes, heart disease, stroke, internal cancers, and other diseases that seem to improve in the presence of sunlight, of which they may well not be getting enough. Because of their genetically higher levels of melanin, they require more sun exposure to produce compounds like vitamin D, and they are less able to store that vitamin for darker days. They have much to gain from the sun and little to fear.
A machine learning algorithm programmed by Dr. Jae Ho Sohn can look at PET scans of human brains and spot indicators of Alzheimer’s disease with a high level of accuracy an average of 6 years before the patients would receive a final clinical diagnosis from a doctor.
To train the algorithm, Sohn fed it images from the Alzheimer’s Disease Neuroimaging Initiative (ADNI), a massive public dataset of PET scans from patients who were eventually diagnosed with either Alzheimer’s disease, mild cognitive impairment or no disorder. Eventually, the algorithm began to learn on its own which features are important for predicting the diagnosis of Alzheimer’s disease and which are not.
Once the algorithm was trained on 1,921 scans, the scientists tested it on two novel datasets to evaluate its performance. The first were 188 images that came from the same ADNI database but had not been presented to the algorithm yet. The second was an entirely novel set of scans from 40 patients who had presented to the UCSF Memory and Aging Center with possible cognitive impairment.
The algorithm performed with flying colors. It correctly identified 92 percent of patients who developed Alzheimer’s disease in the first test set and 98 percent in the second test set. What’s more, it made these correct predictions on average 75.8 months — a little more than six years — before the patient received their final diagnosis.
This is the stuff where AI is going to be totally useful…provided the programs aren’t cheating somehow.
MEL Magazine’s Ian Lecklitner talked to clinical nutritionist David Friedman (author of Food Sanity: How to Eat in a World of Fads and Fiction) about which vegetables Friedman thinks are the healthiest. Happy to see that asparagus is #1:
“This tasty green stalk comes in first place on my vegetable ranking,” Friedman says. “Asparagus is a great source of vitamin K, which helps with blood clotting and building strong bones.” Friedman also mentions that asparagus provides vitamin A (which prevents heart disease), vitamin C (which supports the immune system), vitamin E (which acts as an antioxidant) and vitamin B6 (which, like vitamin A, also prevents heart disease).
Asparagus is also loaded with minerals, including iron (which supports oxygen-carrying red blood cells), copper (which improves energy production) and calcium (which improves bone health). “Asparagus increases your energy levels, protects your skin from sun damage and helps with weight loss,” Friedman continues. “It’s also an excellent source of inulin, a type of carbohydrate that acts as a prebiotic, supporting the growth of health-promoting bacteria in the colon.”
Personal faves brussels sprouts, beets, and broccoli also rank pretty high.
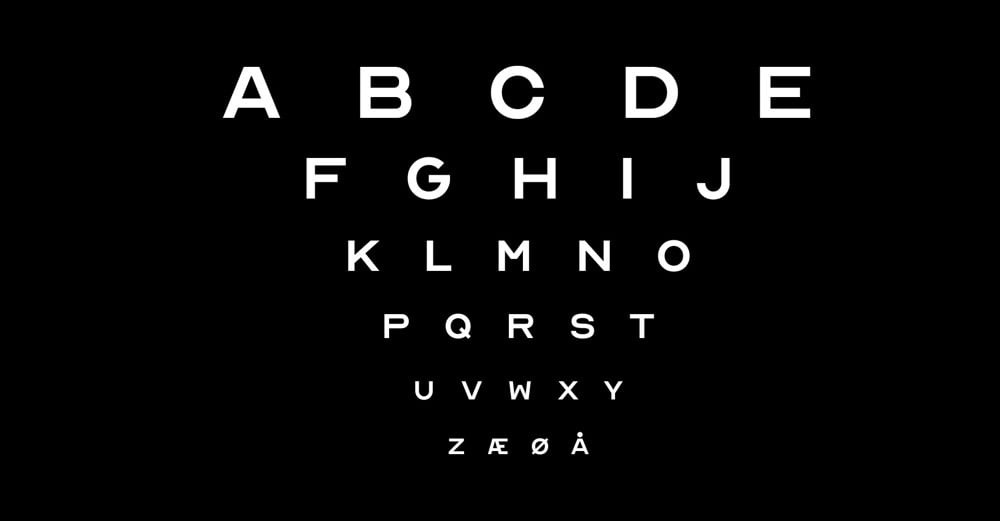
Eye charts at your optometrist’s office typically only have 10 letters on them: CDHKNORSVZ. Inspired by that lettering, creative agency ANTI Hamar and typographer Fábio Duarte Martins have expanded that abbreviated alphabet into a free font with a full alphabet called Optician Sans. Here’s a video look at how they did it:
(via khoi)
For this month’s issue of Topic, palliative care doctor Nathan Gray wrote & illustrated a comic about What Doctors Know About CPR. It does not match what you might have seen on TV.
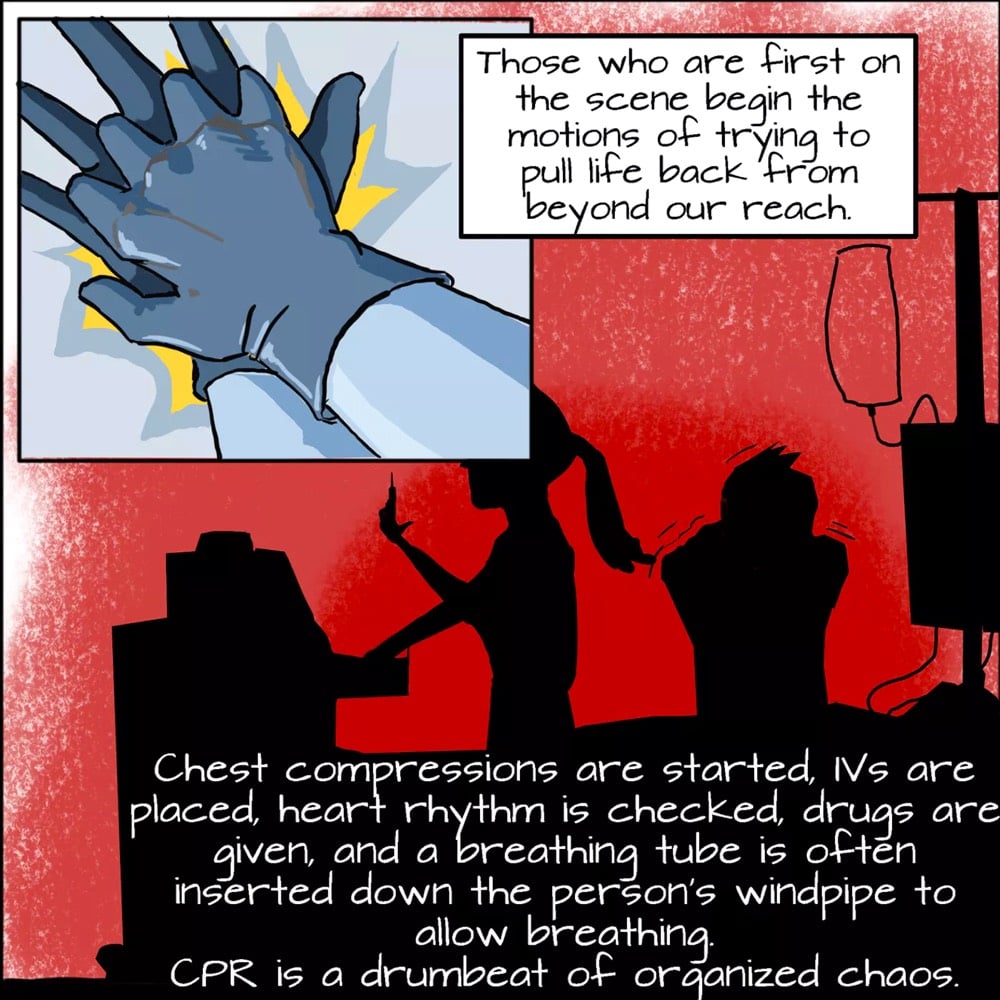
CPR holds an almost sacred space in medicine. Most doctors won’t refuse to perform it, even if they think it will be harmful or useless.
See also a hospital’s playlist of songs for doing perfect CPR chest compressions featuring Crazy in Love, Sweet Home Alabama, and Gloria Gaynor’s I Will Survive.
Nobody writes about health care practice from the inside out like Atul Gawande, here focusing on an increasingly important part of clinical work: information technology.
A 2016 study found that physicians spent about two hours doing computer work for every hour spent face to face with a patient—whatever the brand of medical software. In the examination room, physicians devoted half of their patient time facing the screen to do electronic tasks. And these tasks were spilling over after hours. The University of Wisconsin found that the average workday for its family physicians had grown to eleven and a half hours. The result has been epidemic levels of burnout among clinicians. Forty per cent screen positive for depression, and seven per cent report suicidal thinking—almost double the rate of the general working population.
Something’s gone terribly wrong. Doctors are among the most technology-avid people in society; computerization has simplified tasks in many industries. Yet somehow we’ve reached a point where people in the medical profession actively, viscerally, volubly hate their computers.
It’s not just the workload, but also what Gawande calls “the Revenge of the Ancillaries” — designing software for collaboration between different health care professionals, from surgeons to administrators, all of whom have competing stakes and preferences in how a product is used and designed, what information it offers and what it demands. And most medical software doesn’t handle these competing demands very well.
I don’t know how many people under the age of 35 know about the Chicago Tylenol murders, but for a few weeks in 1982, it was a national news sensation. Seven people in the Chicago area died after ingesting Tylenol capsules laced with potassium cyanide. Retro Report took a look back at this episode, with a focus on how Johnson & Johnson and other drug companies modified their packaging to prevent in-store tampering.
The company considered renaming Tylenol, a word that incorporates some of the letters from 4- (aceTYLamino) phENOL, a chemical name for acetaminophen, the drug’s active ingredient. But a name change was rejected.
Instead, a mere six weeks after the crisis flared, the company offered a different solution, a new bottle with the sorts of safety elements now familiar (if at times exasperating) to every shopper: cotton wad, foil seal, childproof cap, plastic strip. Capsules began to be replaced with caplets the following year.
Johnson & Johnson was viewed as an exemplar of corporate responsibility, and enjoyed what some people described as the greatest comeback since Lazarus. Nowadays, all sorts of products come in containers deemed tamper-proof, or at least tamper-evident, meaning that consumers can readily tell if a seal has been broken or something else is amiss.
Incredibly, the case is still unsolved…no one knows who did it or why. Thinking about the amount of in-store surveillance that we have, it seems unlikely that such a crime would go unsolved for long today.
From an independent newspaper here in Vermont, the heartbreaking and brutally honest obituary of Madelyn Linsenmeir, a 30-year-old mother who died from a drug addiction to opiates that lasted for more a decade.
When she was 16, she moved with her parents from Vermont to Florida to attend a performing arts high school. Soon after she tried OxyContin for the first time at a high school party, and so began a relationship with opiates that would dominate the rest of her life.
It is impossible to capture a person in an obituary, and especially someone whose adult life was largely defined by drug addiction. To some, Maddie was just a junkie — when they saw her addiction, they stopped seeing her. And what a loss for them. Because Maddie was hilarious, and warm, and fearless, and resilient. She could and would talk to anyone, and when you were in her company you wanted to stay. In a system that seems to have hardened itself against addicts and is failing them every day, she befriended and delighted cops, social workers, public defenders and doctors, who advocated for and believed in her ‘til the end. She was adored as a daughter, sister, niece, cousin, friend and mother, and being loved by Madelyn was a constantly astonishing gift.
This is powerfully straightforward writing by Linsenmeir’s family…my condolences are with them. They devoted a few paragraphs at the end of her obit to address addiction and its place in our society:
If you are reading this with judgment, educate yourself about this disease, because that is what it is. It is not a choice or a weakness. And chances are very good that someone you know is struggling with it, and that person needs and deserves your empathy and support.
If you work in one of the many institutions through which addicts often pass — rehabs, hospitals, jails, courts — and treat them with the compassion and respect they deserve, thank you. If instead you see a junkie or thief or liar in front of you rather than a human being in need of help, consider a new profession.
As in many other states, more and more people are dying of opiate overdoses in Vermont even as doctors cut the number of opioid prescriptions they write faster than other areas of the country.
Update: On Facebook, Burlington, VT’s chief of police Brandon del Pozo wrote a response to Linsenmeir’s obituary that is very much worth reading.
Why did it take a grieving relative with a good literary sense to get people to pay attention for a moment and shed a tear when nearly a quarter of a million people have already died in the same way as Maddie as this epidemic grew?
Did readers think this was the first time a beautiful, young, beloved mother from a pastoral state got addicted to Oxy and died from the descent it wrought? And what about the rest of the victims, who weren’t as beautiful and lived in downtrodden cities or the rust belt? They too had mothers who cried for them and blamed themselves.
She died just like my wife’s cousin Meredith died in Bethesda, herself a young mother, but if Maddie was a black guy from the Bronx found dead in his bathroom of an overdose, it wouldn’t matter if the guy’s obituary writer had won the Booker Prize, there wouldn’t be a weepy article in People about it.
Why not?
But if there had been, early enough on, and we acted swiftly, humanely, and accordingly, maybe Maddie would still be here. Make no mistake, no matter who you are or what you look like: Maddie’s bell tolls for someone close to you, and maybe someone you love. Ask the cops and they will tell you: Maddie’s death was nothing special at all. It happens all the time, to people no less loved and needed and human.
(thx, caroline)
If you’re ever called on to perform CPR in an emergency but you don’t have training, the American Heart Association recommends performing “Hands-Only CPR”. There are two easy steps: you call 911 and then you press hard and fast in the center of the person’s chest 100-120 times per minute. As their fact sheet explains, familiar music can help maintain the proper tempo.
Song examples include “Stayin’ Alive” by the Bee Gees, “Crazy in Love” by Beyoncé featuring Jay-Z, “Hips Don’t Lie” by Shakira” or “Walk the Line” by Johnny Cash. People feel more confident performing Hands-Only CPR and are more likely to remember the correct rate when trained to the beat of a familiar song.
When performing CPR, you should push on the chest at a rate of 100 to 120 compressions per minute, which corresponds to the beat of the song examples above.
New York Presbyterian Hospital maintains a Spotify playlist of “Songs to do CPR to” that hit that 100-120 bpm sweet spot.
The playlist includes songs familiar to lifesavers of all generations, from Book of Love by the Monotones to Sweet Home Alabama by Lynyrd Skynyrd to Walk Like an Egyptian by The Bangles to Sorry by Justin Bieber. Stayin’ Alive or Justin Timberlake’s Rock Your Body are probably more appropriate to the situation, but should the need arise, my go-to CPR song is now Crazy in Love. Who knows, Beyoncé might help save someone’s life someday. (via @juliareinstein)
This was a new term for me:
keyword void, or search void, n.: a situation where searching for answers about a keyword returns an absence of authoritative, reliable results, in favor of “content produced by a niche group with a particular agenda.”
An article by Renee DiResta at Wired uses the example of Vitamin K shots, a common treatment given to newborn babies at hospitals, but whose top search results are dominated by anti-vaccination groups.
There’s an asymmetry of passion at work. Which is to say, there’s very little counter-content to surface because it simply doesn’t occur to regular people (or, in this case, actual medical experts) that there’s a need to produce counter-content. Instead, engaging blogs by real moms with adorable children living authentic natural lives rise to the top, stating that doctors are bought by pharma, or simply misinformed, and that the shot is risky and unnecessary. The persuasive writing sounds reasonable, worthy of a second look. And since so much of the information on the first few pages of search results repeats these claims, the message looks like it represents a widely-held point of view. But it doesn’t. It’s wrong, it’s dangerous, and it’s potentially deadly.
I wondered what other examples of keyword voids might be out there, so I searched for it. Unsurprisingly — in retrosepect — you don’t get a lot of relevant results. It’s mostly programming talk, when you literally want a function to return no results.
Science writer Carl Zimmer has a new book on genetics and heredity called She Has Her Mother’s Laugh. The New York Times published an excerpt this week focusing on mosaicism — an unexpected but surprisingly common condition where different cells in the same organism display different DNA (sometimes strikingly, fatally different).
Dr. Walsh and his colleagues have discovered intricate mosaics in the brains of healthy people. In one study, they plucked neurons from the brain of a 17-year-old boy who had died in a car accident. They sequenced the DNA in each neuron and compared it to the DNA in cells from the boy’s liver, heart and lungs.
Every neuron, the researchers found, had hundreds of mutations not found in the other organs. But many of the mutations were shared only by some of the other neurons.
It occurred to Dr. Walsh that he could use the mutations to reconstruct the cell lineages — to learn how they had originated. The researchers used the patterns to draw a sort of genealogy, linking each neuron first to its close cousins and then its more distant relatives.
When they had finished, the scientists found that the cells belonged to five main lineages. The cells in each lineage all inherited the same distinctive mosaic signature.
Even stranger, the scientists found cells in the boy’s heart with the same signature of mutations found in some brain neurons. Other lineages included cells from other organs.
Based on these results, the researchers pieced together a biography of the boy’s brain.
I’ve always been drawn to the idea that each of us are many people, an assembly of mismatched parts, manifesting themselves in different times and contexts. It’s striking to see that reflected, albeit in a refracted way, in our array of possible genomes.
Last month when I posted a video comparing the sizes of various microorganisms, I noted the weirdness of bacteriophages, which are bacteria-killing viruses that look a bit like a 20-sided die stuck on the top of a sci-fi alien’s body.
Bacteriophages are really real and terrifying…if you happen to be a bacteria. Bacteriophages attack by attaching themselves to bacteria, piercing their outer membranes, and then pumping them full of bacteriophage DNA. The phage replicates inside of the bacteria until the bacteria bursts and little baby bacteriophages are exploded out all over the place, ready to attack their own bacteria.
I couldn’t find a good explainer (video or text) about these organisms, but over the weekend, Kurzgesagt rode to the rescue with this video. In the second part of the video, they discuss whether bacteriophages might form the basis of an effective treatment for antibiotic-resistant infections.
A suspect in the Golden State Killer murders has been arrested, based largely on DNA evidence that was apparently obtained in part through creating a dummy profile on a heredity website. California’s laws are apparently fairly permissive when it comes to using familial DNA to match suspects to crimes.
Solving unsolved rape and murder cases is generally good, but turning private websites into repositories of criminal evidence police can obtain without a warrant is generally bad. Like, extra bad.
One of the first things this reminded me of was Cathy O’Neil’s recent call for a Hippocratic Oath for data scientists. The idea is for data scientists to have some ethical guidelines, and above all to avoid doing harm or violating the rights of the people implicated by the practice of data science. In order to do that, you need to bring in the various stakeholders, properly weigh each of their concerns, and continually work to address them.
It’s always an incomplete process, because as O’Neil notes right away, data science isn’t limited to the acts of professional data scientists; it’s also the province of companies, and algorithms, and automated or self-learning uses of data. So in addition to a Hippocratic Oath (or some version of it), you also need a version of HIPAA (the law that guarantees the secure storage and distribution of health information).
DNA/heredity sites seem like the perfect test case for figuring out the compatibility of these two modes of operating. It seems like largely, they’re being treated either as a simple data regime, a la social media networks, and/or under criminal statutes. But a person’s DNA is, or should be, treated like medical information, with strict limits on its use. There has to be some way to figure out how to weigh all of these things together without compromising people’s rights.
This morning I ran across news from two different studies about reducing deaths from opioid overdoses and they both had the same solution: medication-assisted treatment. First, from a study involving inmates in Rhode Island correctional facilities:
The program offers inmates methadone and buprenorphine (opioids that reduce cravings and ease withdrawal symptoms), as well as naltrexone, which blocks people from getting high.
The data set is small but the results are encouraging: there were fewer overdose deaths of former inmates after the program was implemented in 2016.
In the 90s, France used a similar program to cut heroin overdose deaths by 79%:
In 1995, France made it so any doctor could prescribe buprenorphine without any special licensing or training. Buprenorphine, a first-line treatment for opioid addiction, is a medication that reduces cravings for opioids without becoming addictive itself.
With the change in policy, the majority of buprenorphine prescribers in France became primary-care doctors, rather than addiction specialists or psychiatrists. Suddenly, about 10 times as many addicted patients began receiving medication-assisted treatment, and half the country’s heroin users were being treated. Within four years, overdose deaths had declined by 79 percent.
When she was 16, Charlotte Eades was diagnosed with glioblastoma, an extremely aggressive form of brain cancer. About a year after the diagnosis, she began documenting her illness and her life on her YouTube channel. After Eades died, her family made the video above, a short tribute to her life and video blog.
Annie Onishi is a general surgery resident at Columbia University and Wired asked her to break down scenes from movies and TV shows featuring emergency rooms, operating rooms, and other medical incidents. Spoiler alert: if you seek medical treatment from a TV doctor, you will probably die. Secondary spoiler alert: that adrenaline-shot-to-the-heart scene in Pulp Fiction is not as implausible as you might think, even if some of the details are wrong.
Data artist Josh Begley edited together a 5m30s video of every concussion suffered in an NFL game this year. I was barely able to get through this…I had to pause a couple of times. From an article about the video at The Intercept:
The NFL has done a masterful job at mainstreaming the violence of the game, so that fans and spectators don’t feel too bad about what’s actually happening out there. No single word has protected the NFL from the true costs of this violence more than “concussion.” That word puts a protective barrier between us and what’s really going on out on the field.
It’s not a headache. It’s not “getting your bell rung.” You don’t have a bell. It’s a traumatic brain injury. Every single concussion is a new traumatic brain injury. In addition to the torn ACLs and MCLs, in addition to all of the horrible broken bones, the NFL diagnosed at least 281 traumatic brain injuries this season. And no document has ever quite displayed the horror of it all like “Concussion Protocol,” a film by Josh Begley and Field of Vision.
The backwards slow-mo technique is a bit off-putting at first, but as Greg Dorsainville noted in the video’s thread:
If it was in forwards it would be like any big hits package you see in an espn highlight show where we celebrate the football and hit and not mourn the result of the moment: a human in pain, disorientation, and slowly killing themselves.
Having big second thoughts on watching the Super Bowl this weekend, karma offsets or no. (via @harmancipants)
In a study done by UPenn researchers, first-year medical students who were taught art observation classes at the Philadelphia Museum of Art were more proficient at reading clinical imagery than students who didn’t take the classes.
If you’re unfamiliar or uncomfortable with how art and science can mingle to produce something clinically beneficial, it’s a study premise that might seem far-fetched — but it didn’t seem that way to Gurwin, an ophthalmology resident at Penn, in part because she’d already seen the benefits of art education on a medical career firsthand.
“Having studied fine arts myself and having witnessed its impact on my medical training, I knew art observation training would be a beneficial practice in medical school,” she said. “Observing and describing are skills that are taught very well in fine arts training, and so it seemed promising to utilize their teachings and apply it to medicine.”
Gurwin and Binenbaum’s findings, published in the journal Ophthalmology in September: The medical students who’ve dabbled in art just do better.
It’s a glimpse at how non-clinical training can and does make for a better-prepared medical professional. Not only does art observation training improve med students’ abilities to recognize visual cues, it also improves their ability to describe those cues.
The results of this study reminded me of Walter Isaacson’s assertion in his book that Leonardo da Vinci’s greatest skill was his keen observational ability. Not coincidentally, Leonardo was both an artist and a medical researcher who dissected more than 30 human cadavers to study human anatomy. These dissections helped him to represent the human form more realistically in his paintings and drawings.
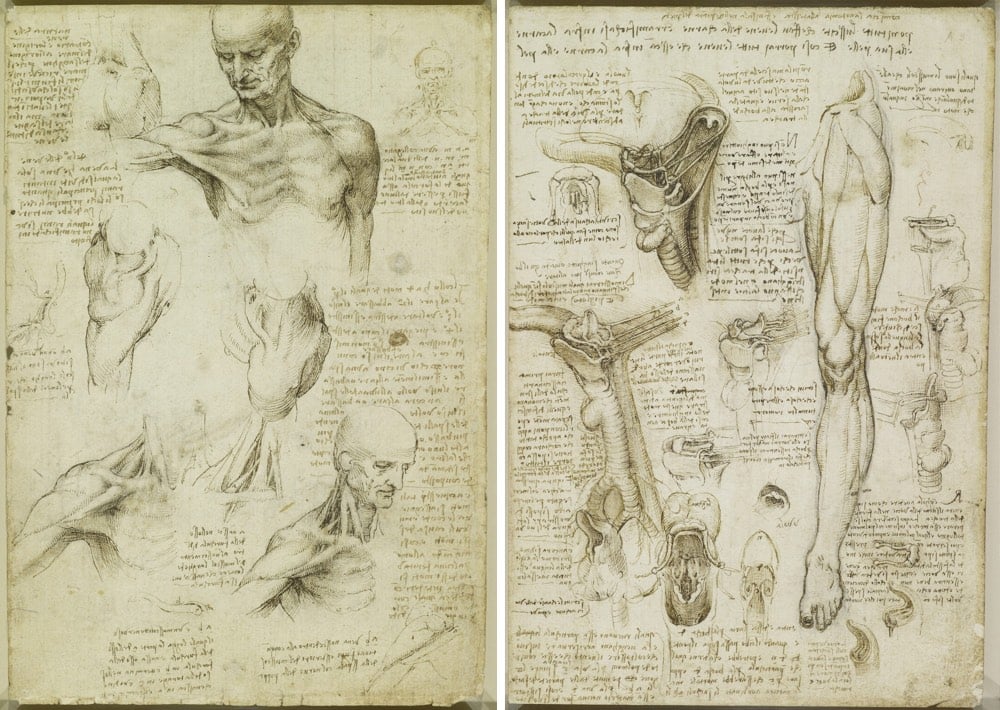
It’s easier to draw a hand, particularly a hand that appears to be moving (as Leonardo liked to do), if you know that’s going on underneath the skin. Looking carefully and purposefully at art, at anatomy, at the physical world, at people’s actions, at movies; it’s all the same skill that can be applied to anything.
I’ve been preoccupied with observation lately…the new kottke.org newsletter is named Noticing for good reason. Again, Leonardo factors in:
Isaacson argues that Leonardo’s observational powers were not innate and that with sufficient practice, we can all observe as he did. People talk in a precious way about genius, creativity, and curiosity as superpowers that people are born with but noticing is a more humble pursuit. Noticing is something we can all do.
In only 90 seconds with the use of a few props (and some profanity), entertainers Penn & Teller offer a succinct and compelling argument of the benefits of vaccinating our children.
So even if vaccination did cause autism, WHICH IT FUCKING DOESN’T, anti-vaccination would still be bullshit.
Along with “Vaccines. And now my kids don’t die.”, this might be my favorite anti-vaxxers broadside ever.
Kurzgesagt takes a look at three possible areas of research that may help people live longer and healthier: senescent cells, NAD+, and stem cells. The distinction articulated early on in the video between optimizing for human lifespan versus increasing human healthspan seems particularly important in this search for a cure for aging.
According to a study published in March 2017 in the Journal of the National Cancer Institute, cancer death rates continue to fall across most cancer types. From 2010 to 2014 (the most recent year that statistical data is available), overall death rates decreased by 1.8%.
Overall cancer death rates from 2010 to 2014 decreased by 1.8% (95% confidence interval [CI] = -1.8% to -1.8%) per year in men, by 1.4% (95% CI = -1.4% to -1.3%) per year in women, and by 1.6% (95% CI = -2.0% to -1.3%) per year in children. Death rates decreased for 11 of the 16 most common cancer types in men and for 13 of the 18 most common cancer types in women, including lung, colorectal, female breast, and prostate, whereas death rates increased for liver (men and women), pancreas (men), brain (men), and uterine cancers.
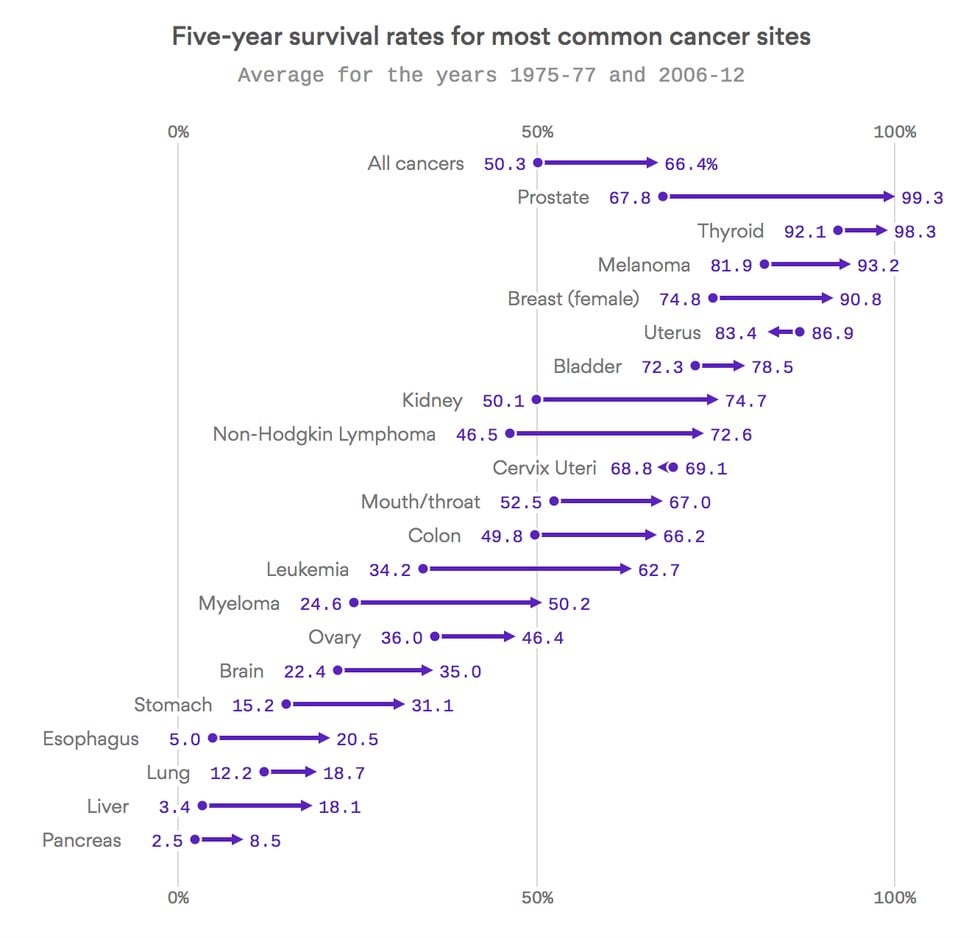
But the trends are much clearer when you look at progress over a longer time period. As this graph from Axios shows, the five-year survival rates for most common types of cancer have increased quite significantly in the past 30-40 years. Survival rates from all cancers increased by 16% and jumped 26% and almost 29% for non-Hodkin lymphoma and leukemia respectively. If you have prostate or thyroid cancer, you’re almost guaranteed to survive 5 years at this point and the female breast cancer survival rate is up to almost 91%. (via @Atul_Gawande)
Currently, the only way to diagnose chronic traumatic encephalopathy (CTE), a disease caused by repeated head trauma, is by posthumously examining brain tissue for signs of tau protein buildup. But a group from Boston University may have found a way to test for CTE in living patients.
McKee and her team discovered a specific biomarker in the brains of former football players. A biomarker is a measurable substance which is, in this case, found in the brain and identifies an abnormality.
This particular biomarker is called CCL11, and it’s a secreted protein the human body uses to help regulate the immune system and inflammation in the body.
As The Ringer’s Claire McNear writes, if a CTE test is easily available to players, what will that do to football? (Or indeed, what will it do to sports like soccer, boxing, skateboarding, or even skiing?)
“After learning all of this,” the retiring Ferguson wrote of the clarity he gained when he began researching CTE, “I feel a bit betrayed by the people or committees put in place by the league who did not have my best interests at heart.” He should feel betrayed, as should many of his fellow players. As will, certainly, so very many, once they have the ability to see what has happened to them. They may wonder, rightfully, about the people who trained them and paid them, sometimes even as they attempted to shut down research into CTE. They may look at the league’s structure, at the lopsided contracts that rob many players of their leverage, forcing them to choose between getting back on the field or losing a paycheck (and possibly getting cut), and at how the league cycles through players like they’re nothing more than easily broken pieces on a board.
Former New England Patriots player Aaron Hernandez, who was serving a life sentence for murdering a friend and who died in prison from suicide earlier this year, was found to have “a severe form” of CTE, a brain disease linked to repeated head trauma that has also been found in many other former NFL players.
Researchers who examined the brain determined it was “the most severe case they had ever seen in someone of Aaron’s age,” said a lawyer for Hernandez in announcing the result at a news conference on Thursday. Hernandez was 27.
Hernandez played three seasons in college and only three in the NFL, yet the damage to his brain was similar to “players with a median age of 67 years”. If you’re a young football player in college or the NFL right now, you have to be looking at this situation pretty hard right now.
See also: Don’t Let Kids Play Football, what the ball boy saw, I’m quitting football, NFL deliberately campaigned against science regarding head injuries, Junior Seau’s family sues NFL over concussions, how professional football might end (sooner than you think), and a message in an NFL player’s suicide.
Former NFL player Ed Cunningham has resigned from his job as a college football color analyst for ABC/ESPN because of “his growing discomfort with the damage being inflicted on the players he was watching each week”.
If Ed Cunningham had not already seen enough, he would be back in a broadcast booth on Saturday afternoon, serving as the color analyst for another top college football game televised on ABC or ESPN. It is the work he has done each fall for nearly 20 years.
But Cunningham, 48, resigned from one of the top jobs in sports broadcasting because of his growing discomfort with the damage being inflicted on the players he was watching each week. The hits kept coming, right in front of him, until Cunningham said he could not, in good conscience, continue his supporting role in football’s multibillion-dollar apparatus.
Another domino falls. Unless there are big changes to the game play, sooner or later football will likely become a marginalized sport in the US.
Senator John McCain has been diagnosed with a particularly aggressive form of brain cancer. The tumor has been removed and McCain is recovering at home with his family. I wish Senator McCain well and hope for a speedy recovery.
In the wake of his diagnosis, many of those expressing support for McCain reference his considerable personal strength in his fight against cancer. President Obama said:
John McCain is an American hero & one of the bravest fighters I’ve ever known. Cancer doesn’t know what it’s up against. Give it hell, John.
McCain’s daughter Meghan references his toughness and fearlessness in a statement released yesterday. Vice-President Joe Biden expressed similar sentiments on Twitter:
John and I have been friends for 40 years. He’s gotten through so much difficulty with so much grace. He is strong — and he will beat this.
This is the right thing to say to those going through something like this, and hearing this encouragement and having the will & energy to meet this challenge will undoubtably increase McCain’s chances of survival. But what Biden said next is perhaps more relevant:
Incredible progress in cancer research and treatment in just the last year offers new promise and new hope. You can win this fight, John.
As with polio, smallpox, measles, and countless other diseases before it, beating cancer is not something an individual can do. Being afflicted with cancer is the individual’s burden to bear but society’s responsibility to cure. In his excellent biography of cancer from 2011, The Emperor of All Maladies, Siddhartha Mukherjee talks about the progress we’ve made on cancer:
Incremental advances can add up to transformative changes. In 2005, an avalanche of papers cascading through the scientific literature converged on a remarkably consistent message — the national physiognomy of cancer had subtly but fundamentally changed. The mortality for nearly every major form of cancer — lung, breast, colon, and prostate — had continuously dropped for fifteen straight years. There had been no single, drastic turn but rather a steady and powerful attrition: mortality had declined by about 1 percent every year. The rate might sound modest, but its cumulative effect was remarkable: between 1990 and 2005, the cancer-specific death rate had dropped nearly 15 percent, a decline unprecedented in the history of the disease. The empire of cancer was still indubitably vast — more than half a million American men and women died of cancer in 2005 — but it was losing power, fraying at its borders.
What precipitated this steady decline? There was no single answer but rather a multitude. For lung cancer, the driver of decline was primarily prevention — a slow attrition in smoking sparked off by the Doll-Hill and Wynder-Graham studies, fueled by the surgeon general’s report, and brought to its full boil by a combination of political activism (the FTC action on warning labels), inventive litigation (the Banzhaf and Cipollone cases), medical advocacy, and countermarketing (the antitobacco advertisements). For colon and cervical cancer, the declines were almost certainly due to the successes of secondary prevention — cancer screening. Colon cancers were detected at earlier and earlier stages in their evolution, often in the premalignant state, and treated with relatively minor surgeries. Cervical cancer screening using Papanicolaou’s smearing technique was being offered at primary-care centers throughout the nation, and as with colon cancer, premalignant lesions were excised using relatively minor surgeries. For leukemia, lymphoma, and testicular cancer, in contrast, the declining numbers reflected the successes of chemotherapeutic treatment. In childhood ALL, cure rates of 80 percent were routinely being achieved. Hodgkin’s disease was similarly curable, and so, too, were some large-cell aggressive lymphomas. Indeed, for Hodgkin’s disease, testicular cancer, and childhood leukemias, the burning question was not how much chemotherapy was curative, but how little: trials were addressing whether milder and less toxic doses of drugs, scaled back from the original protocols, could achieve equivalent cure rates.
Perhaps most symbolically, the decline in breast cancer mortality epitomized the cumulative and collaborative nature of these victories — and the importance of attacking cancer using multiple independent prongs. Between 1990 and 2005, breast cancer mortality had dwindled an unprecedented 24 percent. Three interventions had potentially driven down the breast cancer death rate-mammography (screening to catch early breast cancer and thereby prevent invasive breast cancer), surgery, and adjuvant chemotherapy (chemotherapy after surgery to remove remnant cancer cells).
Understanding how to defeat cancer is an instance where America’s fierce insistence on individualism does us a disservice. Individuals with freedom to pursue their own goals are capable of a great deal, but some problems require massive collective coordination and effort. Beating cancer is a team sport; it can only be defeated by a diverse collection of people and institutions working hard toward the same goal. It will take government-funded research, privately funded research, a strong educational system, philanthropy, and government agencies from around the world working together. This effort also requires a system of healthcare that’s available to everybody, not just to those who can afford it. Although cancer is not a contagious disease like measles or smallpox, the diagnosis and treatment of each and every case brings us closer to understanding how to defeat it. We make this effort together, we spend this time, energy, and money, so that 10, 20, or 30 years from now, our children and grandchildren won’t have to suffer like our friends and family do now.
Newer posts
Older posts
Socials & More