kottke.org posts about vaccines
Dr. Katelyn Jetelina (aka Your Local Epidemiologist) has a frustrating update on how Covid vaccines are probably going to work this fall under the ideologically corrupt Trump regime.
The FDA is expected to license the Covid-19 vaccine. Word is that the label will be restricted to adults 65+ and people at high risk.
The Vaccine Integrity Project and professional organizations likely won’t align with RFK Jr.’s FDA license, which will cause confusion.
If you’re younger than 65 and don’t have a chronic condition, could you still get it after the label change?
Yes, but it will be complicated. While a provider could prescribe it off-label, in practice, it’s likely that most people won’t be able to access it that way.
Jetelina continues:
If you’re under 65 and not high risk, the window to get a Covid-19 vaccine is right now — before the FDA label changes. Once it happens, access will be limited immediately (if it isn’t already). CVS is no longer booking appointments. As far as we know, Walgreens and local pharmacies still are.
That was as of Monday — no idea if that’s still the case. And of course, because this is the United States, insurance will probably be a mess too:
Recommendations from these two organizations are really important for insurers. The hope is they see them and cover all vaccines, regardless of what RFK does. It also provides extra information to physicians who will prescribe off-label if RFK Jr’s FDA changes the label (as expected) this Friday.
We will not know if any of these recommendations affect insurance coverage until insurance companies confirm coverage.
[insert a lot of profanity here; seriously, this makes me so incandescently mad that if I wrote anything more it would contain every fucking swear word I know and then some]
Sources: Aug 18 thread on Bluesky, Aug 20 thread on Bluesky, Aug 18 newsletter.
This is a great data-driven short documentary by Neil Halloran about how smallpox was eradicated from the face of the Earth. And what it took was humanity, through the use of science & humanitarianism, answering its own plea for something to be done about it.
Some philosophers believe there was a secondary humanitarian revolution that followed the scientific revolution. And I note this because the eradication of smallpox also had these two phases. The scientific breakthroughs of inoculation and the vaccine allowed many countries to become virtually smallpox-free — but not all countries. In fact, those 300 to 500 million deaths in the 20th century? They came well after the vaccine had been discovered. So clearly, for much of the world, something more was needed than medical innovation. And fortunately there’s reason to think that these two types of progress might be connected.
Part of being a human is contemplating why some of us get so sick. It’s a practical question and it’s more than that. As we learned about disease, the theory goes that we began to think a little differently about those who fell ill — to see that their suffering truly wasn’t meant to be. We stepped away from thinking it was up to a higher power and into the belief that, well, it was up to us.
See also How smallpox claimed its final victim (I’d never heard this story before watching Halloran’s video), How Children Took the Smallpox Vaccine Around the World, and No One Knows What’s Inside the Smallpox Vaccine.
I loved this short thread from Andrew Miller about how his pediatrician wife helps parents who are skeptical of vaccinating their children change their minds.
So my wife is a pediatrician and works in some hospitals with high vaccine and intervention hesitation (suburban ones). She has found *tremendous* success by just letting the families know she will have to document the higher risk of specific, and often fatal illness, in the chart of their child.
She explains that if their child goes to the ER, the ER might not think to ask about routine newborn care that the parents opted out of, so by putting it in the chart she might be saving the child from this very specific thing. But just as important it makes it feel REAL to the parents.
She identifies and describes the specific thing that their child is now more likely to die from. In detail, including symptoms to watch out for. It’s not abstract. It’s visceral.
From The Economist on the occasion of the award of the Nobel Prize for Medicine to Katalin Karikó and Drew Weissman for their work that led to the development of the Covid-19 mRNA vaccines, a lovely short appreciation of vaccines.
The World Health Organisation (WHO) says that vaccines have saved more from death than any other medical invention. It is a hard claim to gainsay. Vaccines protect people from disease cheaply, reliably and in remarkable numbers. And their capacity to do so continues to grow. In 2021 the who approved a first vaccine against malaria; this week it approved a second.
Vaccines are not only immensely useful; they also embody something beautifully human in their combination of care and communication. Vaccines do not trick the immune system, as is sometimes said; they educate and train it. As a resource of good public health, they allow doctors to whisper words of warning into the cells of their patients. In an age short of trust, this intimacy between government policy and an individual’s immune system is easily misconstrued as a threat. But vaccines are not conspiracies or tools of control: they are molecular loving-kindness.
The WHO says that vaccines currently prevent 4-5 million deaths per year. The CDC points to a paper that says that more than 50 million death can be prevented between 2021 and 2030. Vaccination is nothing short of a scientific miracle. (via eric topol)
From Kurzgesagt, an accessible explanation of what happens to the human body when you get sick.
Your brain activates sickness behavior and reorganizes your body’s priorities to defense. The first thing you notice is that your energy level drops and you get sleepy. You feel apathetic, often anxious or down and you lose your appetite. Your sensitivity to pain is heightened and you seek out rest. All of this serves to save your energy and reroute it into your immune response.
They also reveal the best way to boost your immune system to protect yourself against disease. I don’t want to spoil it but it’s vaccines. Vaccines are one of the best things humans have ever invented.
From Vox’s Joss Fong, a video essay on how conservatives turned against the Covid-19 vaccine in the US.
President Donald Trump presided over the fastest vaccine development process in history, leading to abundant, free vaccines in the US by the spring of 2021. Although the mRNA Covid-19 vaccines haven’t been able to stop transmission of the virus, they have been highly effective against hospitalization and death, saving hundreds of thousands of lives and rendering the majority of new Covid-19 deaths preventable.
Trump has received three doses of the vaccine. But many of his most dedicated supporters have refused, and many have died as a result. Why? Obvious culprits include misinformation on social media and Fox News and the election of Joe Biden, which placed a Democrat at the top of the US government throughout the vaccine distribution period. But if you look closely at the data, you’ll see that vaccine-hesitant conservatives largely made up their mind well before the vaccines were available and before Donald Trump lost the 2020 election.
Fong makes a compelling argument for the potential genesis of conservative vaccine denial: early on in the pandemic, in February and March 2020, prominent conservative leaders and media outlets (like Trump and Fox News) told their constituents that the threat of the pandemic and of SARS-CoV-2 has been exaggerated by journalists and liberal politicians. So, in the mind of a Fox News viewer, if the pandemic is not such a big deal, if it is “just the flu”, then why would you want to get vaccinated? Or wear a mask? Or take any precautions whatsoever? Or, most certainly, why wouldn’t you be angry at you and your kids (your kids!) being forced to do any of those things?
Historically, contracting the measles has been linked to subsequent illness (and possibly death) from other causes. In the past few years, scientists have discovered why this is: measles causes “immune amnesia”.
Enter “immune amnesia”, a mysterious phenomenon that’s been with us for millennia, though it was only discovered in 2012. Essentially, when you’re infected with measles, your immune system abruptly forgets every pathogen it’s ever encountered before — every cold, every bout of flu, every exposure to bacteria or viruses in the environment, every vaccination. The loss is near-total and permanent. Once the measles infection is over, current evidence suggests that your body has to re-learn what’s good and what’s bad almost from scratch.
“In a way, infection of the measles virus basically sets the immune system to default mode,” says Mansour Haeryfar, a professor of immunology at Western University, Canada, “as if it has never encountered any microbes in the past”.
This re-learning process takes up to three years, which “around the time it takes infants to acquire immunity to everyday pathogens in the first place”. In the meantime…
It’s not surprising, then, that measles doesn’t just increase the risk of illness, but also death. In fact, childhood mortality from other viruses is strongly linked to the incidence of measles. The 2015 study showed that when childhood mortality in the UK, US, or Denmark goes up, this is usually because measles has become more prevalent.
The findings explain why vaccinating children against measles has the unexpected, beneficial side-effect of reducing deaths among children, way beyond the numbers who were ever at risk of dying from measles itself.
Of course, an extremely effective and safe vaccine offers protection against both measles and the immune amnesia it causes. But with the steep rise in anti-vaccination sentiment during the pandemic and the increasing willingness of conservative leaders to disregard public health protections in favor of “individual freedom”, widely vaccinating against this dangerous pathogen in the US & elsewhere will be more difficult than in the past.
From Max Roser at Our World in Data: Our history is a battle against the microbes: we lost terribly before science, public health, and vaccines allowed us to protect ourselves.
Science is the foundation for our success. 150 years ago nobody knew where diseases came from. Or more precisely, people thought they knew, but they were wrong. The widely accepted idea at the time was the ‘Miasma’ theory of disease. Miasma, the theory held, was a form of “bad air” that causes disease. The word malaria is testament to the idea that ‘mal aria’ — ‘bad air’ in medieval Italian — is the cause of the disease.
Thanks to the work of a number of doctors and chemists in the second half of the 19th century humanity learned that not noxious air, but specific germs cause infectious diseases. The germ theory of disease was the breakthrough in the fight against the microbe. Scientists identified the pathogens that cause the different diseases and thereby laid the foundation for perhaps the most important technical innovation in our fight against them: vaccines.
Here’s what vaccines did for us, in three charts:
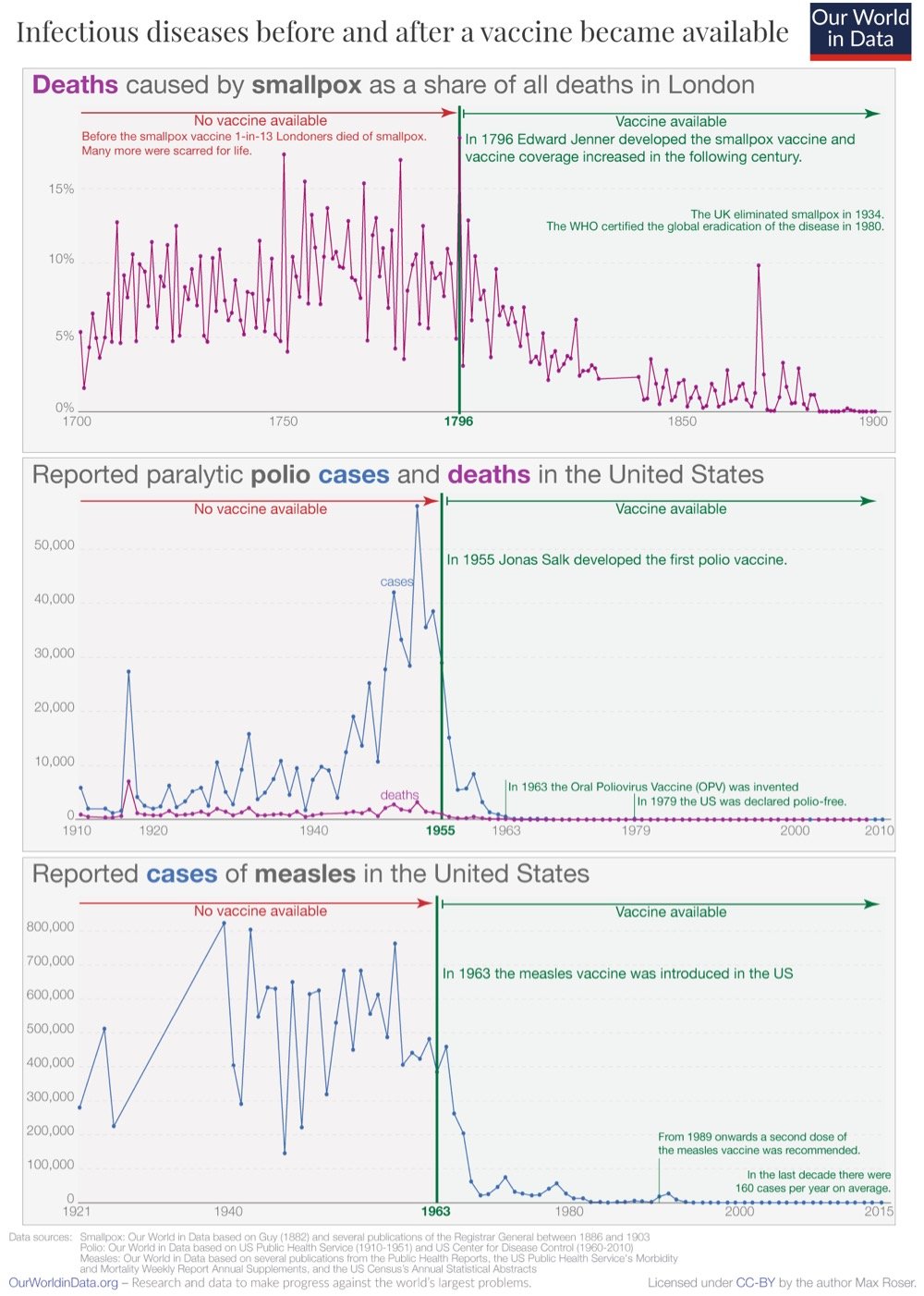
Even among those who accept and understand how good vaccines are at stopping disease, it’s difficult to truly appreciate just how incredible and transformative they have been. By one estimate, vaccines saved between 150 & 200 million lives from 1980 & 2018…and that’s just for smallpox. Covid-19 vaccines have saved hundreds of thousands of lives in Europe and the US in the first year of their availability. Truly a miraculous invention.
This is such an interesting article on vaccine avoidance in America by a primary care doctor & sociologist who have studied the phenomenon in America and other places. As more data has come in about the pandemic and vaccination program, the main differentiator in whether someone is willing to get a vaccine or not is class.
Over the past four decades, governments have slashed budgets and privatized basic services. This has two important consequences for public health. First, people are unlikely to trust institutions that do little for them. And second, public health is no longer viewed as a collective endeavor, based on the principle of social solidarity and mutual obligation. People are conditioned to believe they’re on their own and responsible only for themselves. That means an important source of vaccine hesitancy is the erosion of the idea of a common good.
Americans began thinking about health care decisions this way only recently; during the 1950s polio campaigns, for example, most people saw vaccination as a civic duty. But as the public purse shrunk in the 1980s, politicians insisted that it’s no longer the government’s job to ensure people’s well-being; instead, Americans were to be responsible only for themselves and their own bodies. Entire industries, such as self-help and health foods, have sprung up on the principle that the key to good health lies in individuals making the right choices.
Almost more than anything else, the pandemic has shown how damaged the US is from decades of neglect of the common good and how vulnerable we are to things like disease and political coups.
It may seem like sometimes that with the pandemic, we’re back to square one. With the much more contagious Delta variant in play and an increasing number of breakthrough infections, the efficacy of these vaccines that we thought were amazing maybe aren’t? (Or maybe we just need to readjust our expectations?) But in terms of what these vaccines were specifically developed for — reducing & preventing severe disease and death — they are still very much doing their job. Just take a look at this graph from a White House Covid-19 press briefing yesterday:
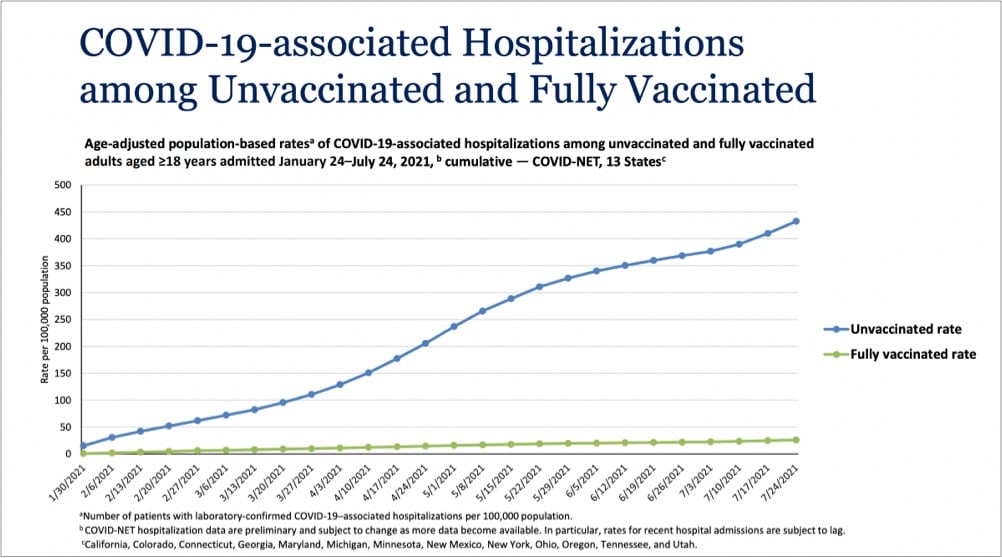
Even with Delta endemic in the country, the vaccines are providing extraordinary protection against infections severe enough to land folks in the hospital. In a recent CDC study of infections and hospitalizations in Los Angeles County, they report that on July 25, the hospitalization rate of unvaccinated people was 29.2 times that of fully vaccinated persons. 29 times the protection is astounding for a medical intervention. These vaccines work, we’re lucky to have them, and we need to get as many people worldwide as we can vaccinated as quickly as we can. Period.
You might want to take a deep breath or do a couple of laps around the house before watching this video about a community in the Ozarks with a very low Covid-19 vaccination rate. Here’s a sample. An ICU patient wearing an oxygen mask on why he didn’t get vaccinated:
I’m more of a libertarian and I don’t like being told what I have to do. I’m still not completely 100% sold on the inoculation.
Video narrator:
It was eerie to hear Christopher insist on his individual freedoms even as he struggled to breathe.
Can you hear me screaming all the way from my desk to wherever you are? I don’t like being told what I have to do?! Fucking hell. And this:
There’s no better place to see the impact of this political rhetoric than in the hospital. Only about 50 percent of the staff are vaccinated. None of the unvaccinated staffers were willing to talk.
Absolutely maddening. I want off this ride.
For The Atlantic, Katherine Wu writes about the difficulty of communicating how vaccines work and how they protect individuals and communities from disease: Vaccines Are Like Sunscreen… No, Wait, Airbags… No, Wait…
Unfortunately, communal benefit is harder to define, harder to quantify, and harder to describe than individual protection, because “it’s not the way Americans are used to thinking about things,” Neil Lewis, a behavioral scientist and communications expert at Cornell, told me. That’s in part because communal risk isn’t characteristic of the health perils people in wealthy countries are accustomed to facing: heart disease, stroke, diabetes, cancer. Maybe that’s part of why we gravitate toward individual-focused comparisons. Slipping into a pandemic-compatible, population-based frame of mind is a big shift. In the age of COVID-19, “there’s been a lot of focus on the individual,” Lewis told me. That’s pretty at odds “with how infection works.”
As someone who has struggled with analogizing the virus & vaccines, I was nodding my head a lot while reading this. Something I’ve noticed in recent years that Wu didn’t get into is that readers desire precision in metaphors and analogies, even though metaphor is — by definition! — not supposed to be taken literally. People seem much more interested in taking analogies apart, identifying what doesn’t work, and discarding them rather than — more generously and constructively IMO — using them as the author intended to better understand the subject matter. The perfect metaphor doesn’t exist because then it wouldn’t be a metaphor.
The Panola Project is a short film by Rachael DeCruz and Jeremy Levine that follows the efforts of local convenience store owner Dorothy Oliver to get the people in her small Alabama community vaccinated against Covid-19. A trusted member of her community, Oliver teams up with county commissioner Drucilla Russ-Jackson to call & go door-to-door, talking with people one-on-one, cajoling and telling personal stories of loss to get folks signed up for a mobile vaccination clinic.
In the film, Oliver and Russ-Jackson arrange for a hospital to set up a pop-up site in Panola, but the site will only be established if they get at least forty people to sign up to take the vaccine. We follow Oliver as she goes door to door, talking people into signing up, lightly cajoling them about their fears and concerns. When I asked her how she does it, her answer was disarmingly simple: “I just be nice to them,” she said. “I don’t go at them saying, ‘You gotta do that.’” DeCruz, too, was struck by the way Oliver and Jackson talked to people who were on the fence about the vaccine, an issue more often discussed with stridency of various types. “There’s this very warm and kind of loving and caring way that Dorothy and Ms. Jackson approached those conversations, even when people aren’t in agreement. And it wasn’t done in a way that’s, like, ‘I know better than you.’ “
Oliver’s charm with the skeptics is remarkable, but so is her determination to bring the vaccine to her underserved town. Most of the women and men Oliver talked to leaped at the opportunity to sign up for the vaccine. On vaccine day, they rolled down their car windows to thank her. “We appreciate y’all giving it to us, because a lot of people don’t really know where to go to take these vaccines,” one woman tells her. Vaccine hesitancy in Black communities has been harped on in the media, but those conversations can gloss over questions of availability. Levine told me that they were struck by how many people had put off vaccination for logistical rather than ideological reasons. In Panola, he says, they regularly heard people say, “I want the shot. How do I get this? I don’t have a car; how am I going to get forty miles to the closest hospital and back?”
The result? In a state with one of the lowest vaccination rates in the country, 94% of adults in Panola have been vaccinated, due in part to Oliver’s and Russ-Jackson’s efforts.
Charles Gaba has been graphing the Covid-19 vaccination rates of the 50 states (and DC) against the percentage of people who voted for Donald Trump in 2020 and there is unsurprisingly a clear correlation between the two:
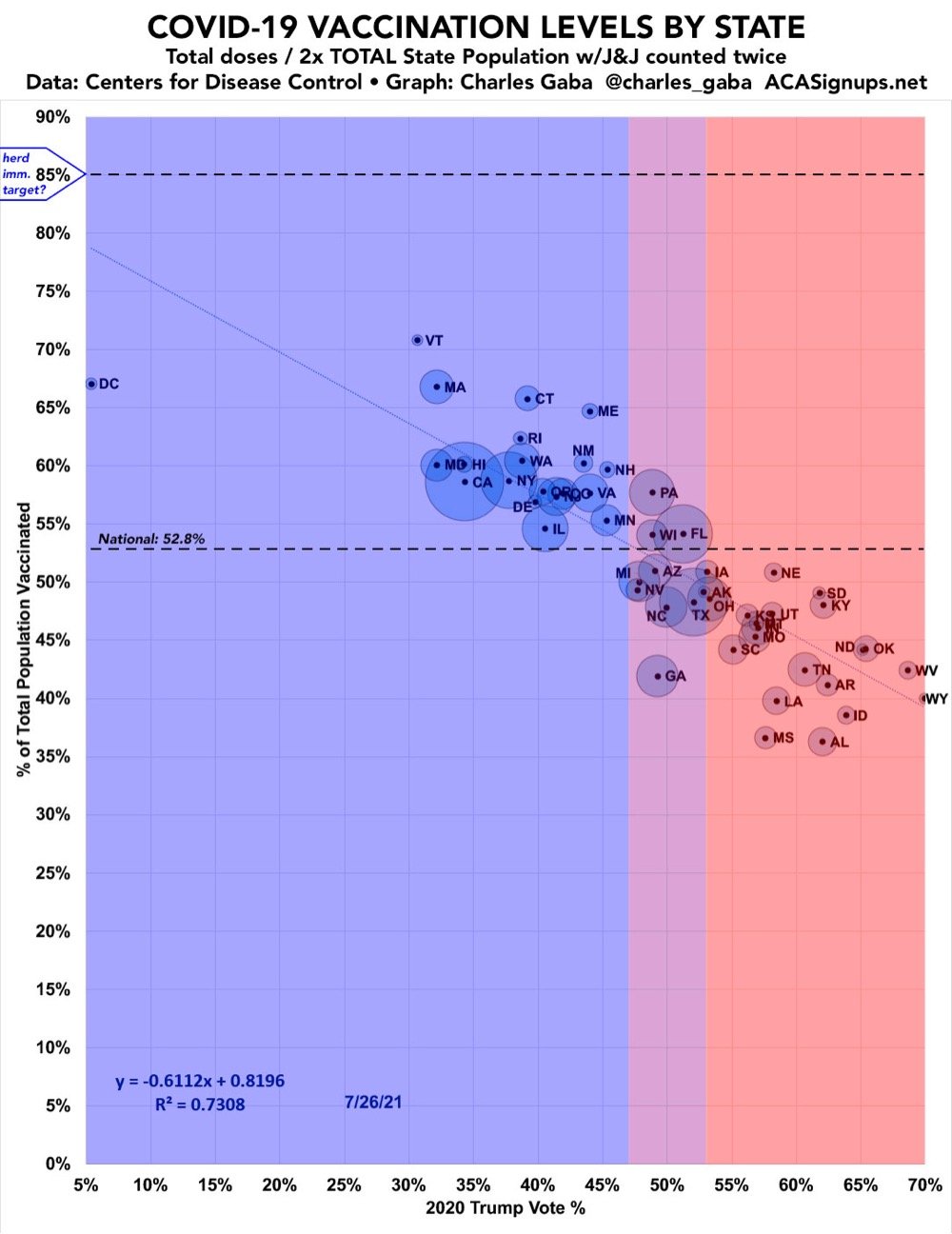
As one commenter noted, all of the solidly “blue” states are above the vaxxed national average and all the solidly “red” states are below it. The picture is a little more muddy when you look at the rates at the county level:
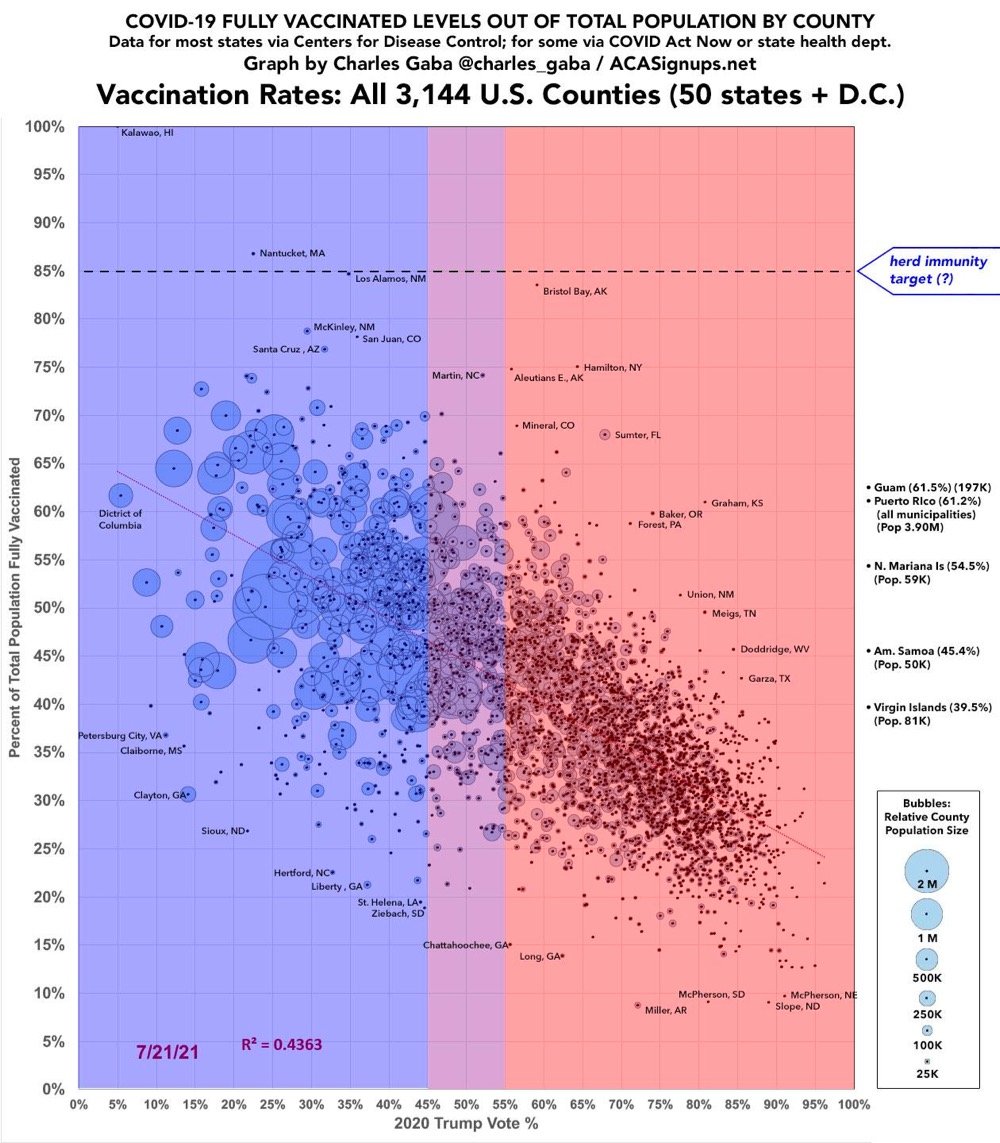
The “conservatives are unvaxxed” trend is still there, but a lack of access and education around the vaccines in counties with large Black and Latino populations also plays a large role in whether people are vaccinated or not.
Dr. Brytney Cobia treats Covid-19 patients at the Grandview Medical Center in Birmingham, Alabama, a state that ranks last in the US in fully vaccinated adults. In a recent Facebook post, Cobia shares that people are willing to get vaccinated after having to watch an unvaccinated member of their family die from Covid.
I’ve made a LOT of progress encouraging people to get vaccinated lately!!! Do you want to know how? I’m admitting young healthy people to the hospital with very serious COVID infections. One of the last things they do before they’re intubated is beg me for the vaccine. I hold their hand and tell them that I’m sorry, but it’s too late. A few days later when I call time of death, I hug their family members and I tell them the best way to honor their loved one is to go get vaccinated and encourage everyone they know to do the same. They cry. And they tell me they didn’t know. They thought it was a hoax. They thought it was political. They thought because they had a certain blood type or a certain skin color they wouldn’t get as sick. They thought it was ‘just the flu’. But they were wrong. And they wish they could go back. But they can’t. So they thank me and they go get the vaccine. And I go back to my office, write their death note, and say a small prayer that this loss will save more lives.
Heartbreaking.
Since yesterday’s announcement, I’d been feeling uneasy about the CDC’s decision to update its guidance to state that fully vaccinated people don’t need to wear masks in most situations indoors or out. Zeynep Tufekci’s piece in the Times nails why.
It’s difficult for officials to issue rules as conditions evolve and uncertainty continues. So I hesitate to question the agency’s approach. But it’s not clear whether it was responding to scientific evidence or public clamor to lift state and local mandates, which the C.D.C. said could remain in place.
It might have been better to have kept up indoor mask mandates to help suppress the virus for maybe as little as a few more weeks.
The C.D.C. could have set metrics to measure such progress, saying that guidelines would be maintained until the number of cases or the number vaccinations reached a certain level, determined by epidemiologists.
The vaccine is on its way to controlling Covid-19 in the US — but we’re not there yet. We’re not the UK or Israel…they’re further along in their vaccination campaigns and their daily cases and deaths are way down, warranting behavioral changes. In the US, over 600 people/day are still dying of Covid-19 and our case positivity rate is still above 3%. Too many people, including almost all children, are still vulnerable and as Tufekci says, the CDC could have waited a few more weeks to more quickly drive down the virus levels.
Update: The CDC’s move has been sharply condemned by National Nurses United, the nation’s largest union of registered nurses:
“The union noted that more than 35,000 new cases of coronavirus were being reported each day and that more than 600 people were dying each day. “Now is not the time to relax protective measures, and we are outraged that the C.D.C. has done just that while we are still in the midst of the deadliest pandemic in a century,” Ms. Castillo said.”
And Ken Schultz notes that the needle the CDC is trying to thread here might not work out the way that they’d hoped.
Imagine the social preference ordering is:
1. Unvaccinated wear masks, vaccinated don’t.
2. Everyone wears masks.
3. No one wears masks.
Selfish, short-sighted behavior and the inability to monitor vaccination status mean that, in trying to get #1, you can end up at #3.
So I trust the CDC’s position that #1 is socially desirable from a scientific perspective. But by undermining mask mandates, they have made it more likely that we end up in #3, which science says is still risky. Living with #2 for now respects both science and social science.
In 1955, epidemiologist Thomas Francis Jr. announced the results of a field trial of the polio vaccine that Jonas Salk had developed. America erupted in joy.
Now a phalanx of bulky television cameras focussed on Francis as he prepared to report on the efficacy of the vaccine. He had good news to share: to cheers from the audience, he explained that the Salk vaccine was sixty to seventy per cent effective against the most prevalent strain of poliovirus, and ninety per cent effective against the other, less common strains. All this had been shown through what was, at that time, the largest vaccine trial ever conducted.
All afternoon and evening, church bells rang out across America. People flooded into the streets, kissing and embracing; parents hugged their kids with joy and relief. Salk became an instant national hero, turning down the offer of a ticker-tape parade in New York City; President Dwight D. Eisenhower invited him to the White House and, later, asked Congress to award him a Congressional Gold Medal. That night, from the kitchen of a colleague’s house, Salk — whose name was being touted in newspapers, magazines, radio reports, and television news broadcasts around the world — gave his first network-TV interview to Edward R. Murrow, whose show “See It Now” had exposed the tactics of Senator Joseph McCarthy a year earlier. Blushing in admiration, Murrow asked the doctor, “Who owns the patent on this vaccine?” “The people,” Salk said, nobly. “There is no patent. Could you patent the sun?”
In the days that followed, schoolchildren were instructed by their teachers to write thank-you notes to Salk. Universities lined up to offer him honorary degrees. Millions of American doctors, nurses, and parents got down to the serious business of vaccinating their children against polio, using a shot they’d been anticipating for seventeen years.
But the polio vaccine rollout had its challenges, including a manufacturing negligence & oversight failure that resulted in tens of thousands of polio cases in otherwise healthy children.
In May, the polio vaccination drive was temporarily suspended. Leonard Scheele, the U.S. Surgeon General, inspected the facilities of all six vaccine companies and fired the government officials he considered to be culpable; the director of the N.I.H. and the Secretary of Health voluntarily resigned. New safety procedures were developed, including an improved means of filtering the viral mix just before the formaldehyde was added. Better tests were developed to detect live virus, and stricter record-keeping was instituted. The incident could have created a vaccine-hesitancy crisis. But, incredibly, the American public readily accepted the medical establishment’s explanation for the failure, and its pledges to right the situation. The nation’s trust in medical progress and in Dr. Salk was so resolute that, when it was announced that a new, safe polio vaccine was available, parents pushed their children back to the head of the line. It’s hard to imagine such an outcome today.
This is a very good and bracing essay from David Roth for Defector about a certain type of knee-jerk libertarian response to the pandemic in the US.
In place of any actually ennobling liberty or more fundamental freedom, contemporary American life mostly offers choices. But since most of these are not really choices at all in any meaningful way, it might be more accurate to say that we’re offered selection. The choice between paying for health insurance and running up six figures of non-dischargeable debt because you got sick, for instance, is honestly less a choice than a hostage situation. But because the second outcome is still extremely possible even if you choose to pay for health insurance, it’s more correct to say that the choice is already made, and that the decision is more about choosing from an array of variously insufficient and predatory options the one whose name or price or risk you like most. Sometimes there isn’t even that, and the choice is a binary one between something and nothing. None of this is really what anyone would choose, but these ugly individuated choices are what we get.
And then:
The broader complacent and unreasoned acceptance that props up our otherwise untenable status quo is shot through all these facile “it’s a private matter and a personal choice” formulations; if you have accepted that mostly useless choices between dreary outcomes are all you could ever get as a citizen in the wealthiest and most powerful country on earth, then you have also accepted that these choices are actually very important, and that making them is the thing makes you free. None of these personal choices actually make anything better for the person making them. In the case of the vaccine, those choices have devastating downstream impacts for all the people who glance off the choice-maker as they carve their personal hero’s journeys through the world. None of this matters as much as the idea that the choice is theirs to make.
The NY Times has a profile of Dr. Katalin Kariko, who struggled for decades against a system unwilling to consider and fund her ideas about how messenger RNA could be used to instruct cells inside human bodies to “make their own medicines”. Her work has culminated in two highly effective vaccines for Covid-19 and is being extended to produce possible vaccines for HIV, the flu, tuberculosis, and malaria.
Now Katalin Kariko, 66, known to colleagues as Kati, has emerged as one of the heroes of Covid-19 vaccine development. Her work, with her close collaborator, Dr. Drew Weissman of the University of Pennsylvania, laid the foundation for the stunningly successful vaccines made by Pfizer-BioNTech and Moderna.
For her entire career, Dr. Kariko has focused on messenger RNA, or mRNA — the genetic script that carries DNA instructions to each cell’s protein-making machinery. She was convinced mRNA could be used to instruct cells to make their own medicines, including vaccines.
Stat also wrote a piece about Kariko and the development of the mRNA vaccines. It seems like Kariko will be strongly considered for a Nobel Prize in Chemistry for her achievements. The Covid vaccines will save hundreds of thousands of lives alone, and if mRNA can indeed be harnessed to protect against HIV and malaria, the effect on the world will be immense. Give Kariko all the prizes and whatever she wants to be happy in life — she’s earned it and more.
Update: From Derek Thompson at The Atlantic, How mRNA Technology Could Change the World.
But mRNA’s story likely will not end with COVID-19: Its potential stretches far beyond this pandemic. This year, a team at Yale patented a similar RNA-based technology to vaccinate against malaria, perhaps the world’s most devastating disease. Because mRNA is so easy to edit, Pfizer says that it is planning to use it against seasonal flu, which mutates constantly and kills hundreds of thousands of people around the world every year. The company that partnered with Pfizer last year, BioNTech, is developing individualized therapies that would create on-demand proteins associated with specific tumors to teach the body to fight off advanced cancer. In mouse trials, synthetic-mRNA therapies have been shown to slow and reverse the effects of multiple sclerosis. “I’m fully convinced now even more than before that mRNA can be broadly transformational,” Özlem Türeci, BioNTech’s chief medical officer, told me. “In principle, everything you can do with protein can be substituted by mRNA.”
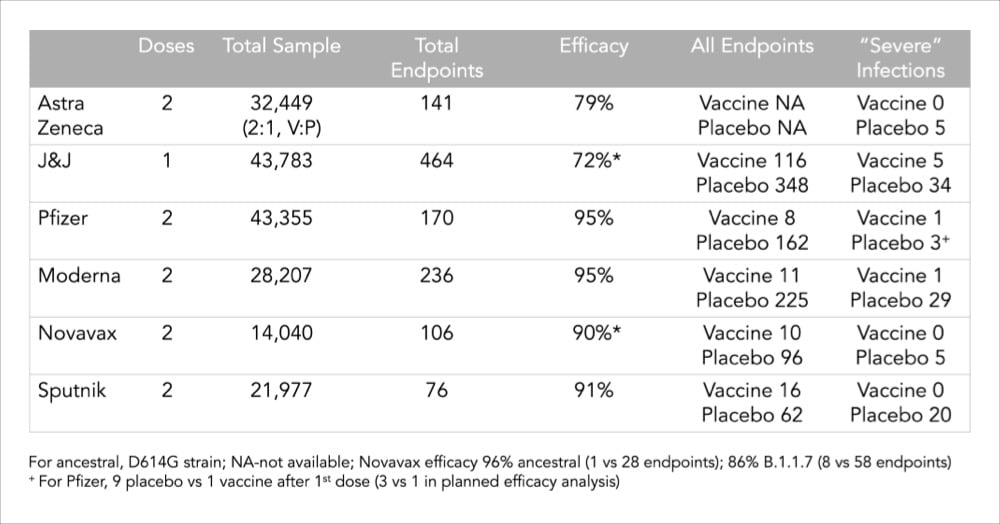
Related to my post from last month about what a 95% or 66% efficacy rate of a vaccine even means, Vox made a clear and concise video about why comparing vaccine efficacy rates is difficult — trials were done in different countries with different variants under different conditions with different levels of disease — and why protection against severe illness, hospitalization and death is a better way to compare and evaluate these vaccines. As this chart from Dr. Eric Topol shows, all of the major vaccines show strong protection against severe illness.
I thought this interview with Dr. Ashish K. Jha, dean of the Brown University School of Public Health, was really good and useful in terms of calibrating expectations with regard to the “end” of the pandemic, vaccines, and variants. On the guidance that vaccinated people should be getting:
I think it is essential that we give guidance to people. And I think we should give guidance to people on what they can do safely once they are vaccinated. People say, “Can your behavior change?” My answer is: absolutely! That’s a major motivation for getting vaccinated. First of all, what’s very clear to me is vaccinated people hanging out with other vaccinated people is pretty darn close to normal. You don’t have to wear a mask. You can share a meal. The chance that a fully vaccinated person will transmit the virus to another fully vaccinated person who then will get sick and die … I mean, sure, people get struck by lightning, too. But you don’t make policy based on that. And we need to remind people that there is a huge benefit to getting vaccinated, which is that you are safe enough to do the things you love with other vaccinated people.
After getting his second dose of the Covid-19 vaccine at a clinic at Berkshire Community College, Yo-Yo Ma got out his cello and performed a 15-minute impromptu concert for the others folks at the clinic.
When Ma had first visited the clinic for his first shot, he did so quietly, taking in the surroundings, staff said. But brought his cello when he returned for the second shot.
Staff described how a hush fell across the clinic as Ma began to play. “It was so weird how peaceful the whole building became, just having a little bit of music in the background,” said Leslie Drager, the lead clinical manager for the vaccination site, according to the Washington Post.
Why is it weird? Music is amazing. I know you could never get such a “frivolous” spending measure through an American deliberative body these days, but how awesome would it be for the government to commission out-of-work musicians to play at vaccination clinics? Ok maybe you couldn’t have anyone sing and the brass & woodwinds would probably have to sit this one out, but you could have strings, guitars, percussion, pianos, DJs, etc. there to play some relaxing, uplifting, or energetic music, according to local custom & culture. Bring back the WPA!
According to a study conducted by the Pew Research Center, among those people who said they probably or definitely won’t get a Covid-19 vaccine, the top two reasons given were “concern about side effects” and “the vaccines were developed and tested too quickly”. For our purposes here, I’m going to ignore the first concern — the data is pretty conclusive that, on average, the vaccine side effects are minimal when compared to the effects of actually contracting Covid-19 — and focus on the quick development timeline. If you’re among those who are apprehensive about the unprecedented speed at which the world’s governments and scientific community mobilized to create several effective Covid-19 vaccines, I hope the following will help you make a good decision.
In reading a bunch of different resources (linked below throughout), I identified six main reasons why the Covid-19 vaccines were developed so quickly compared to past efforts.
1. The need was urgent. Covid-19 changed the entire world in a very short span of time and it was evident in the absence of an effective vaccine, tens of millions more people would unnecessarily die and/or suffer and the rest of us would be living in fear of disease and death. This urgency drove several of the other factors here: the availability of funding, resources, and collaboration.
2. Funding & focus. Companies and governments threw billions and billions of dollars at this. Companies, research centers, and scientists dropped other stuff they were working on to study SARS-CoV-2 and Covid-19. Governments prioritized regulatory approval for trials, etc. From a thread by Dr. Kat Arney:
Relatively few in the scientific, pharma & policy worlds care about vaccines compared w/ drugs. Most vaccine programmes are underfunded as they’re perceived as not profitable, only relevant to LMICs, & have few research groups/companies working on them. Getting funding & research capacity for vax usually takes months/years. COVID-19 vaccine was a massive global research effort w/ $millions for multiple groups/projects in weeks. Years of funding cycles & lab research happened in months, huge amount of time saved.
And from a presentation given by Dr. Anthony Fauci:
We proceeded at risk. So people say, what do you mean by “at risk”? Are you risking safety? Are you risking scientific integrity? No, it’s a financial risk. In other words, you invest in things that cost a lot of money before you even have an answer to whether the prior step worked.
And a classic example is the production of large scale amounts of clinical lots, which have been produced and are being produced before you even know that your vaccine works, so that you have hundreds of millions of doses ready to go. If the vaccine works, you’ve saved many months. If the vaccine doesn’t, you lost a lot of money, to the tune of hundreds of millions if not billions of dollars. But it was felt it was worth that investment and that risk financially in order to save time.
More on that here. As Dr. Faheem Younus put it, “We didn’t cut corners; we cut the crap!”
3. Availability of volunteers & high incidence of disease. In order to statistically show the vaccine works, you need people to test it on and you need enough people in the studies to get sick. Kat Arney again:
To show vax effectiveness, you need a high number of people with the disease in the population — big problem with the Ebola vax is that it took so long to develop the outbreak was over & the couldn’t get enough numbers to conclusively show it worked
We’re in a global pandemic — the vaccine is being tested in places with very high community prevalence, so trials can hit pre-determined statistical milestones very quickly. Huge amount of time saved.
Hundreds of thousands of people around the world volunteered to test these vaccines — without them, we’d be months and years away from a safe, tested vaccine.
4. International & corporate collaboration. Countries and companies shared research, data, and resources because the primary goal was to develop effective vaccines and save lives, not make a profit. For instance, Chinese researchers posted the genome for SARS-CoV-2 on January 11, 2020, allowing the effort to develop a vaccine to begin.
5. We knew a lot about coronaviruses from previous work. This wasn’t an effort that started from scratch. From Bloomberg:
The Pfizer-BioNTech and Moderna vaccines may seem brand new, but they are the culmination of more than a decade of work that started during the SARS and MERS outbreaks. Vaccines were even developed against MERS but were never needed. Nevertheless, scientists learned a huge amount from working with that virus, which is from the same family as the one that causes Covid-19.
From Dr. Habibul Ahsan:
Really, most of the vaccine platform development work is already done. You just have to do the remaining part, which is adding the right viral antigens to the already-proven platform and making sure it’s safe and effective in humans. Even in just the last five to 10 years, we’ve made big leaps in developing new kinds of vaccine platforms like those being tested for SARS-CoV-2.
6. Scientific and technological capability. Ok, we know a lot about coronaviruses but humanity’s general scientific and technological abilities have never been stronger or more powerful. Again from Bloomberg:
Remember also that technology has evolved rapidly — for example, we’re now about able to sequence the genomes of every mutant version of the virus in less than a day. That helps in speeding up vaccine development.
Dr. Mark Toshner sums up the effort:
However we have collectively now shown that with money no object, some clever and highly motivated people, an unlimited pool of altruistic volunteers, and sensible regulators that we can do amazing things.
Further reading: The lightning-fast quest for COVID vaccines — and what it means for other diseases (Nature), How were researchers able to develop COVID-19 vaccines so quickly? (Univ. of Chicago), The race for the COVID-19 vaccine: A story of innovation and collaboration (Carnall Farrar), COVID-19 vaccines: development, evaluation, approval and monitoring (European Medicines Agency).
Stat’s Andrew Joseph and Helen Branswell on the short-term, middle-term, and long-term future of the coronavirus in the US. The short-term outlook is dominated by vaccination & variants; some parts of the country will continue to be affected by outbreaks:
Conditions may be ripe for a better summer, however. Vaccine supplies should be flowing more freely, at least in the U.S.; the Biden administration now expects enough vaccine doses in hand for all adults by the end of May. With most vulnerable populations protected, there should be fewer hospitalizations and deaths. And with warmer weather, people can return to outdoor life.
Widespread transmission of the virus could be replaced by more sporadic and localized outbreaks. There’s also growing evidence that vaccines don’t just protect people from getting symptomatic Covid-19, but can reduce transmission.
And in the long-term, well, SARS-CoV-2 will be around for years and even decades to come:
Years from now, SARS-CoV-2 could join the ranks of OC43, 229E, NL63, and HKU1 — the four endemic, seasonal coronaviruses that cause a chunk of common colds every year. Essentially, our immune systems — primed by vaccines, boosters, and previous encounters with the coronavirus — will be ready to knock back SARS-2 when we see it again, potentially blocking an infection or leading to one that causes no symptoms or maybe just the sniffles.
It’s good to read stuff like this — it provides a basis to use when calibrating your optimism or pessimism for future activities and desires.

In the 70s, the US government enlisted the droids of Star Wars to encourage parents to immunize their kids against childhood diseases like whooping cough and measles.
American parents weren’t getting their kids vaccinated. Measles, polio and whooping cough were taking a toll on young lives. Just as it is today, the message was important but the spot itself was horrible — a sludgy, if informative script. We shot it in a faux sci-fi control room. Most memorable was the way R2 appeared to pay no attention to the laws of physics.
(via kottke ride home)
After the Biden administration announced they will have enough Covid-19 vaccine supply to cover every single adult in the country by the end of May, I got to wondering about what they were going to do with the tens & hundreds of millions of surplus doses already procured for the remainder of the year. “Oh,” I thought, naively, “We’ll be able to distribute it to countries that can’t easily procure or manufacture vaccines of their own!” And I’m sure some of that will happen, if only for PR purposes. But it’s perhaps more likely that America will practice vaccine diplomacy and use the stockpile to reestablish its global leadership.
The United States has backed away from the world. This isn’t a Clinton thing or a W Bush thing or an Obama thing or a Trump thing or a Biden thing, but instead a United States thing. The American people lost interest in playing a constructive role in the world three decades ago, and America’s political leadership has molded itself around that fact. Trump may have been instinctually and publicly hostile to all things international, but Biden is only different in tone. Biden’s Buy-American program is actually more anti-globalization than Trump’s America-First rhetoric as it is an express violation of most of America’s international trade commitments. TeamBiden says it wants to reestablish America’s global leadership…but it plans to do so without any troops or money. Sorry, but that’s not how it works.
Which makes the possibilities for vaccine diplomacy wildly interesting. The United States has no responsibility to provide COVID vaccines to the world. It can — it will — distribute them, but it will want something in return.
Even if you disagree with some of the analysis here, it will be interesting to watch where America’s stockpile ends up. Given Biden’s rhetoric of “listening to the science” when it comes to the pandemic, I hope that at least some of that supply goes to places that need it most to make certain the pandemic doesn’t sputter on for years, generating potentially dangerous new variants, even if it’s politically disadvantageous.
Update: Countries now scrambling for COVID-19 vaccines may soon have surpluses to donate by Jon Cohen and Kai Kupferschmidt for Science magazine:
Like three dozen other countries, the United States contracted with multiple vaccine companies for several times the number of doses needed to cover its population. No one knew at the time which, if any, of the candidate vaccines would work or when they might prove safe and effective. But by now, most of the prepurchased vaccines appear to offer solid protection — which means many countries will receive far more vaccine than they need. The excess doses the United States alone may have by July would vaccinate at least 200 million people.
A chart in the article notes that the US has procured enough vaccine to cover almost 1.5 billion people after fully vaccinating its entire population.
In popular press and social media, there’s been a misunderstanding of what is actually meant when scientists say that the Pfizer and Moderna Covid-19 vaccines have an efficacy of 94-95%. It does not mean that 95% of vaccinated people are protected from infection — these vaccines are better than that. Dr. Piero Olliaro explains in a letter to The Lancet:
The mRNA-based Pfizer and Moderna vaccines were shown to have 94-95% efficacy in preventing symptomatic COVID-19, calculated as 100 x (1 minus the attack rate with vaccine divided by the attack rate with placebo). It means that in a population such as the one enrolled in the trials, with a cumulated COVID-19 attack rate over a period of 3 months of about 1% without a vaccine, we would expect roughly 0.05% of vaccinated people would get diseased.
Another way to put it: you’re 20 times less likely to get Covid-19 with a vaccine than without. (And again, data indicates these are safe vaccines.) Olliaro explains with some simple math:
If we vaccinated a population of 100,000 and protected 95% of them, that would leave 5000 individuals diseased over 3 months, which is almost the current overall COVID-19 case rate in the UK. Rather, a 95% vaccine efficacy means that instead of 1000 COVID-19 cases in a population of 100,000 without vaccine (from the placebo arm of the abovementioned trials, approximately 1% would be ill with COVID-19 and 99% would not) we would expect 50 cases (99.95% of the population is disease-free, at least for 3 months).
And of course if you vaccinate widely, it becomes a compounding situation because the virus just runs out of people to infect.
In an opinion piece for the NY Times, Zeynep Tufekci and epidemiologist Michael Mina are urging for new trials of the Moderna and Pfizer/BioNTech Covid-19 vaccines to begin immediately to see how effective a single dose might be in preventing new infections. If the trials do indicate that a single dose works, that would effectively double the number of people we could vaccinate within a certain time period, saving countless lives in the US and worldwide.
Both vaccines are supposed to be administered in two doses, a prime and a booster, 21 days apart for Pfizer and 28 days for Moderna. However, in data provided to the F.D.A., there are clues for a tantalizing possibility: that even a single dose may provide significant levels of protection against the disease.
If that’s shown to be the case, this would be a game changer, allowing us to vaccinate up to twice the number of people and greatly alleviating the suffering not just in the United States, but also in countries where vaccine shortages may take years to resolve.
But to get there — to test this possibility — we must act fast and must quickly acquire more data.
For both vaccines, the sharp drop in disease in the vaccinated group started about 10 to 14 days after the first dose, before receiving the second. Moderna reported the initial dose to be 92.1 percent efficacious in preventing Covid-19 starting two weeks after the initial shot, when the immune system effects from the vaccine kick in, before the second injection on the 28th day
That raises the question of whether we should already be administrating only a single dose. But while the data is suggestive, it is also limited; important questions remain, and approval would require high standards and more trials.
The piece concludes: “The possibility of adding hundreds of millions to those who can be vaccinated immediately in the coming year is not something to be dismissed.”
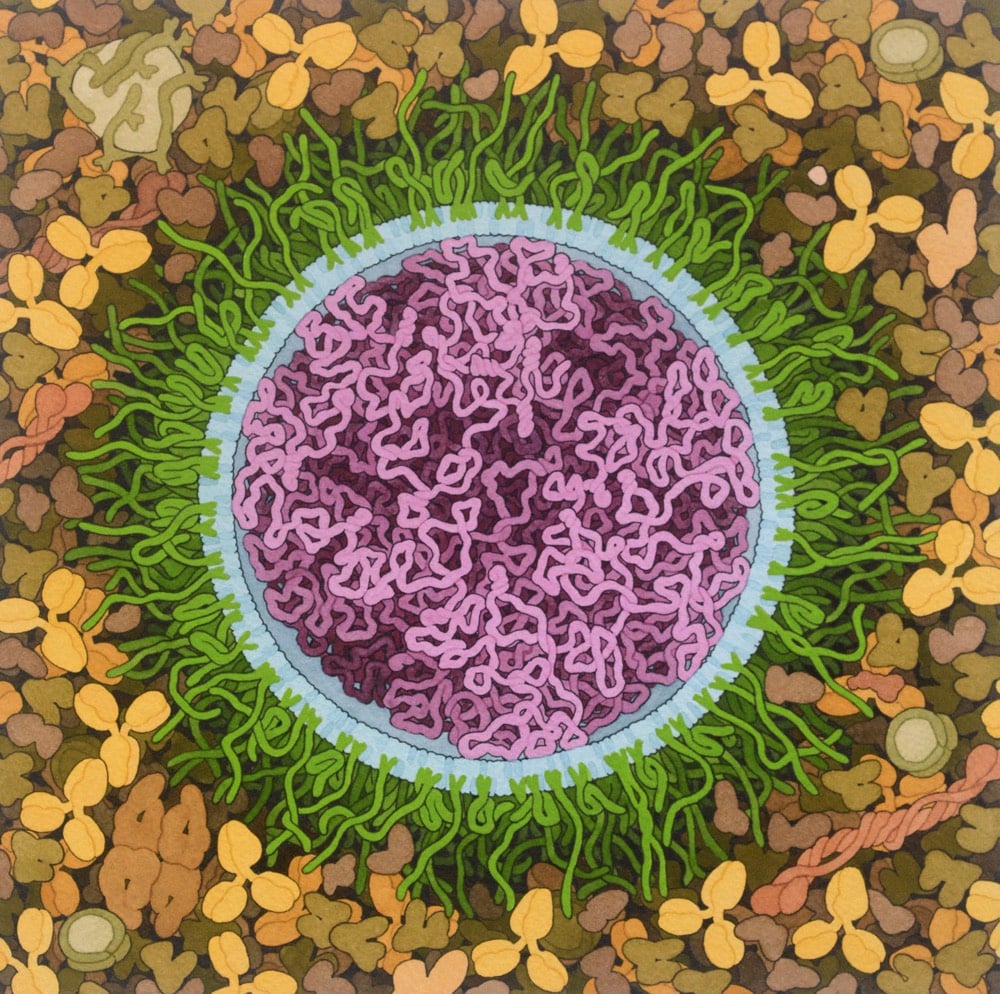
Artist and biologist David Goodsell has done a painting of the Covid-19 mRNA vaccine.
The vaccine structure is highly idealized, with spike mRNA in magenta, lipids in blue, and PEG-lipid in green. The background is blood serum or lymph.
Both the Pfizer/BioNTech and the Moderna Covid-19 vaccines are based on mRNA — you can brush up on how they work at Stat or the CDC.
mRNA vaccines are a new type of vaccine to protect against infectious diseases. To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, they teach our cells how to make a protein — or even just a piece of a protein — that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.
See also Goodsell’s painting of a SARS coronavirus from back in February.
Older posts


Socials & More