kottke.org posts about science
I thought this interview with Dr. Ashish K. Jha, dean of the Brown University School of Public Health, was really good and useful in terms of calibrating expectations with regard to the “end” of the pandemic, vaccines, and variants. On the guidance that vaccinated people should be getting:
I think it is essential that we give guidance to people. And I think we should give guidance to people on what they can do safely once they are vaccinated. People say, “Can your behavior change?” My answer is: absolutely! That’s a major motivation for getting vaccinated. First of all, what’s very clear to me is vaccinated people hanging out with other vaccinated people is pretty darn close to normal. You don’t have to wear a mask. You can share a meal. The chance that a fully vaccinated person will transmit the virus to another fully vaccinated person who then will get sick and die … I mean, sure, people get struck by lightning, too. But you don’t make policy based on that. And we need to remind people that there is a huge benefit to getting vaccinated, which is that you are safe enough to do the things you love with other vaccinated people.
According to a study conducted by the Pew Research Center, among those people who said they probably or definitely won’t get a Covid-19 vaccine, the top two reasons given were “concern about side effects” and “the vaccines were developed and tested too quickly”. For our purposes here, I’m going to ignore the first concern — the data is pretty conclusive that, on average, the vaccine side effects are minimal when compared to the effects of actually contracting Covid-19 — and focus on the quick development timeline. If you’re among those who are apprehensive about the unprecedented speed at which the world’s governments and scientific community mobilized to create several effective Covid-19 vaccines, I hope the following will help you make a good decision.
In reading a bunch of different resources (linked below throughout), I identified six main reasons why the Covid-19 vaccines were developed so quickly compared to past efforts.
1. The need was urgent. Covid-19 changed the entire world in a very short span of time and it was evident in the absence of an effective vaccine, tens of millions more people would unnecessarily die and/or suffer and the rest of us would be living in fear of disease and death. This urgency drove several of the other factors here: the availability of funding, resources, and collaboration.
2. Funding & focus. Companies and governments threw billions and billions of dollars at this. Companies, research centers, and scientists dropped other stuff they were working on to study SARS-CoV-2 and Covid-19. Governments prioritized regulatory approval for trials, etc. From a thread by Dr. Kat Arney:
Relatively few in the scientific, pharma & policy worlds care about vaccines compared w/ drugs. Most vaccine programmes are underfunded as they’re perceived as not profitable, only relevant to LMICs, & have few research groups/companies working on them. Getting funding & research capacity for vax usually takes months/years. COVID-19 vaccine was a massive global research effort w/ $millions for multiple groups/projects in weeks. Years of funding cycles & lab research happened in months, huge amount of time saved.
And from a presentation given by Dr. Anthony Fauci:
We proceeded at risk. So people say, what do you mean by “at risk”? Are you risking safety? Are you risking scientific integrity? No, it’s a financial risk. In other words, you invest in things that cost a lot of money before you even have an answer to whether the prior step worked.
And a classic example is the production of large scale amounts of clinical lots, which have been produced and are being produced before you even know that your vaccine works, so that you have hundreds of millions of doses ready to go. If the vaccine works, you’ve saved many months. If the vaccine doesn’t, you lost a lot of money, to the tune of hundreds of millions if not billions of dollars. But it was felt it was worth that investment and that risk financially in order to save time.
More on that here. As Dr. Faheem Younus put it, “We didn’t cut corners; we cut the crap!”
3. Availability of volunteers & high incidence of disease. In order to statistically show the vaccine works, you need people to test it on and you need enough people in the studies to get sick. Kat Arney again:
To show vax effectiveness, you need a high number of people with the disease in the population — big problem with the Ebola vax is that it took so long to develop the outbreak was over & the couldn’t get enough numbers to conclusively show it worked
We’re in a global pandemic — the vaccine is being tested in places with very high community prevalence, so trials can hit pre-determined statistical milestones very quickly. Huge amount of time saved.
Hundreds of thousands of people around the world volunteered to test these vaccines — without them, we’d be months and years away from a safe, tested vaccine.
4. International & corporate collaboration. Countries and companies shared research, data, and resources because the primary goal was to develop effective vaccines and save lives, not make a profit. For instance, Chinese researchers posted the genome for SARS-CoV-2 on January 11, 2020, allowing the effort to develop a vaccine to begin.
5. We knew a lot about coronaviruses from previous work. This wasn’t an effort that started from scratch. From Bloomberg:
The Pfizer-BioNTech and Moderna vaccines may seem brand new, but they are the culmination of more than a decade of work that started during the SARS and MERS outbreaks. Vaccines were even developed against MERS but were never needed. Nevertheless, scientists learned a huge amount from working with that virus, which is from the same family as the one that causes Covid-19.
From Dr. Habibul Ahsan:
Really, most of the vaccine platform development work is already done. You just have to do the remaining part, which is adding the right viral antigens to the already-proven platform and making sure it’s safe and effective in humans. Even in just the last five to 10 years, we’ve made big leaps in developing new kinds of vaccine platforms like those being tested for SARS-CoV-2.
6. Scientific and technological capability. Ok, we know a lot about coronaviruses but humanity’s general scientific and technological abilities have never been stronger or more powerful. Again from Bloomberg:
Remember also that technology has evolved rapidly — for example, we’re now about able to sequence the genomes of every mutant version of the virus in less than a day. That helps in speeding up vaccine development.
Dr. Mark Toshner sums up the effort:
However we have collectively now shown that with money no object, some clever and highly motivated people, an unlimited pool of altruistic volunteers, and sensible regulators that we can do amazing things.
Further reading: The lightning-fast quest for COVID vaccines — and what it means for other diseases (Nature), How were researchers able to develop COVID-19 vaccines so quickly? (Univ. of Chicago), The race for the COVID-19 vaccine: A story of innovation and collaboration (Carnall Farrar), COVID-19 vaccines: development, evaluation, approval and monitoring (European Medicines Agency).
Stat’s Andrew Joseph and Helen Branswell on the short-term, middle-term, and long-term future of the coronavirus in the US. The short-term outlook is dominated by vaccination & variants; some parts of the country will continue to be affected by outbreaks:
Conditions may be ripe for a better summer, however. Vaccine supplies should be flowing more freely, at least in the U.S.; the Biden administration now expects enough vaccine doses in hand for all adults by the end of May. With most vulnerable populations protected, there should be fewer hospitalizations and deaths. And with warmer weather, people can return to outdoor life.
Widespread transmission of the virus could be replaced by more sporadic and localized outbreaks. There’s also growing evidence that vaccines don’t just protect people from getting symptomatic Covid-19, but can reduce transmission.
And in the long-term, well, SARS-CoV-2 will be around for years and even decades to come:
Years from now, SARS-CoV-2 could join the ranks of OC43, 229E, NL63, and HKU1 — the four endemic, seasonal coronaviruses that cause a chunk of common colds every year. Essentially, our immune systems — primed by vaccines, boosters, and previous encounters with the coronavirus — will be ready to knock back SARS-2 when we see it again, potentially blocking an infection or leading to one that causes no symptoms or maybe just the sniffles.
It’s good to read stuff like this — it provides a basis to use when calibrating your optimism or pessimism for future activities and desires.
After the Biden administration announced they will have enough Covid-19 vaccine supply to cover every single adult in the country by the end of May, I got to wondering about what they were going to do with the tens & hundreds of millions of surplus doses already procured for the remainder of the year. “Oh,” I thought, naively, “We’ll be able to distribute it to countries that can’t easily procure or manufacture vaccines of their own!” And I’m sure some of that will happen, if only for PR purposes. But it’s perhaps more likely that America will practice vaccine diplomacy and use the stockpile to reestablish its global leadership.
The United States has backed away from the world. This isn’t a Clinton thing or a W Bush thing or an Obama thing or a Trump thing or a Biden thing, but instead a United States thing. The American people lost interest in playing a constructive role in the world three decades ago, and America’s political leadership has molded itself around that fact. Trump may have been instinctually and publicly hostile to all things international, but Biden is only different in tone. Biden’s Buy-American program is actually more anti-globalization than Trump’s America-First rhetoric as it is an express violation of most of America’s international trade commitments. TeamBiden says it wants to reestablish America’s global leadership…but it plans to do so without any troops or money. Sorry, but that’s not how it works.
Which makes the possibilities for vaccine diplomacy wildly interesting. The United States has no responsibility to provide COVID vaccines to the world. It can — it will — distribute them, but it will want something in return.
Even if you disagree with some of the analysis here, it will be interesting to watch where America’s stockpile ends up. Given Biden’s rhetoric of “listening to the science” when it comes to the pandemic, I hope that at least some of that supply goes to places that need it most to make certain the pandemic doesn’t sputter on for years, generating potentially dangerous new variants, even if it’s politically disadvantageous.
Update: Countries now scrambling for COVID-19 vaccines may soon have surpluses to donate by Jon Cohen and Kai Kupferschmidt for Science magazine:
Like three dozen other countries, the United States contracted with multiple vaccine companies for several times the number of doses needed to cover its population. No one knew at the time which, if any, of the candidate vaccines would work or when they might prove safe and effective. But by now, most of the prepurchased vaccines appear to offer solid protection — which means many countries will receive far more vaccine than they need. The excess doses the United States alone may have by July would vaccinate at least 200 million people.
A chart in the article notes that the US has procured enough vaccine to cover almost 1.5 billion people after fully vaccinating its entire population.
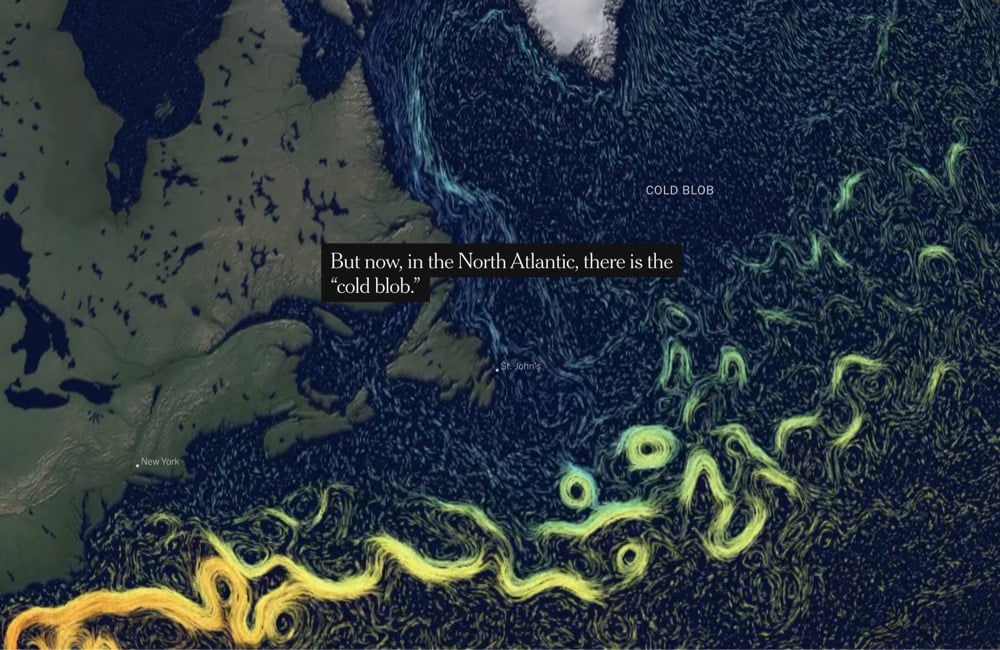
The NY Times has a fantastic interactive piece about a particularly disturbing aspect of the climate crisis: the evidence that a huge Atlantic circulation pattern is weakening and could collapse, leading to “a monstrous change” in temperature, precipitation, and other chaotic effects across the globe.
Now, a spate of studies, including one published last week, suggests this northern portion of the Gulf Stream and the deep ocean currents it’s connected to may be slowing. Pushing the bounds of oceanography, scientists have slung necklace-like sensor arrays across the Atlantic to better understand the complex network of currents that the Gulf Stream belongs to, not only at the surface, but hundreds of feet deep.
“We’re all wishing it’s not true,” Peter de Menocal, a paleoceanographer and president and director of the Woods Hole Oceanographic Institution, said of the changing ocean currents. “Because if that happens, it’s just a monstrous change.”
The consequences could include faster sea level rise along parts of the Eastern United States and parts of Europe, stronger hurricanes barreling into the Southeastern United States, and perhaps most ominously, reduced rainfall across the Sahel, a semi-arid swath of land running the width of Africa that is already a geopolitical tinderbox.
One of the potential reasons for this weakening is that the quickly melting Greenland ice sheet is dumping massive amounts of cold fresh water into the North Atlantic, disrupting the Gulf Stream. This is “the cold blob”.
The northern arm of the Gulf Stream is but one tentacle of a larger, ocean-spanning tangle of currents called the Atlantic Meridional Overturning Circulation, or AMOC. Scientists have strong evidence from ice and sediment cores that the AMOC has weakened and shut down before in the past 13,000 years. As a result, mean temperatures in parts of Europe may have rapidly dropped to about 15 degrees Celsius below today’s averages, ushering in arctic like conditions. Parts of northern Africa and northern South America became much drier. Rainfall may even have declined as far away as what is now China. And some of these changes may have occurred in a matter of decades, maybe less.
The AMOC is thus a poster child for the idea of climatic “tipping points” — of hard-to-predict thresholds in Earth’s climate system that, once crossed, have rapid, cascading effects far beyond the corner of the globe where they occur. “It’s a switch,” said Dr. de Menocal, and one that can be thrown quickly.
Which brings us to the cold blob. Almost everywhere around the world, average temperatures are rising — except southeast of Greenland where a large patch of the North Atlantic has become colder in recent years.
The title of this post references a “frozen Europe” but because the Earth is a nonlinear system, a weakened AMOC could actually have the opposite effect:
Scientists at the U.K.’s National Oceanography Centre have somewhat counterintuitively linked the cold blob in the North Atlantic with summer heat waves in Europe. In 2015 and 2018, the jet stream, a river of wind that moves from west to east over temperate latitudes in the northern hemisphere, made an unusual detour to the south around the cold blob. The wrinkle in atmospheric flow brought hotter-than-usual air into Europe, they contend, breaking temperature records.
“That was not predicted,” said Joel Hirschi, principal scientist at the centre and senior author of the research. It highlights how current seasonal forecasting models are unable to predict these warm summers. And it underscores the paradox that, far from ushering in a frigid future for, say, Paris, a cooler North Atlantic might actually make France’s summers more like Morocco’s.
(thx, meg)
Using an x-ray technique, MIT researchers have digitally unfolded and read 17th-century letters that had been “letterlocked” by their authors to prevent them from being read in transit. Reading the letters in this way allows close study without actually unfolding and potentially damaging these letters or altering them against further study. This is a fully digital image of one of the unlocked letters:

From a NY Times piece about the research:
In an interview, Jana Dambrogio, the study’s lead author and a conservator at the M.I.T. Libraries, said that learning of the trove’s existence inspired her to see if more technologically inclined colleagues could find a way to digitally open the locked letters. At the time, in 2014, scholars could read and study such letters only by cutting them open, which often damaged the documents and obscured or eliminated clues as to how they had been secured.
“We really need to keep the originals,” Ms. Dambrogio said. “You can keep learning from them, especially if you keep the locked packets closed.”
The old letters were protected from prying eyes when the sheets of writing paper were carefully folded to become their own secure enclosures.
The first step of their digital opening is to scan a target letter with an advanced X-ray machine. The resulting three-dimensional image — much like a medical scan — reveals the letter’s internal configuration. A computer then analyzes the image to undo the folds and, almost magically, turn the layers into a flat sheet, revealing handwritten text that can be read.
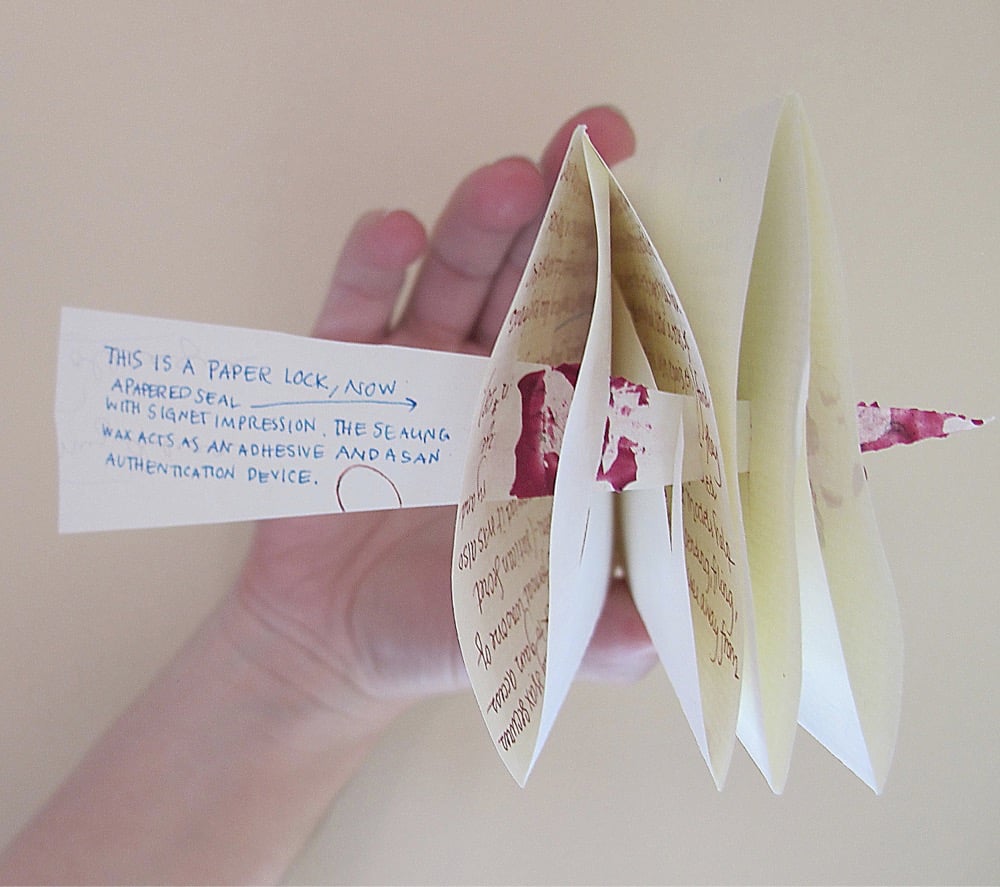
Here’s a contemporary example of the letterlocking technique where folds, slits, and wax are used to lock the letter and provide authentication:
A letterlocking technique in action, modeled after a triangle-locked letter sent by Sir Francis Walsingham in 1587:
Whoa and this spiral-locked letter modeled on a message sent by Queen Elizabeth I to France’s Henry III in the 1570s:
And this is a list of all the letterlocking techniques and formats the researchers have identified:
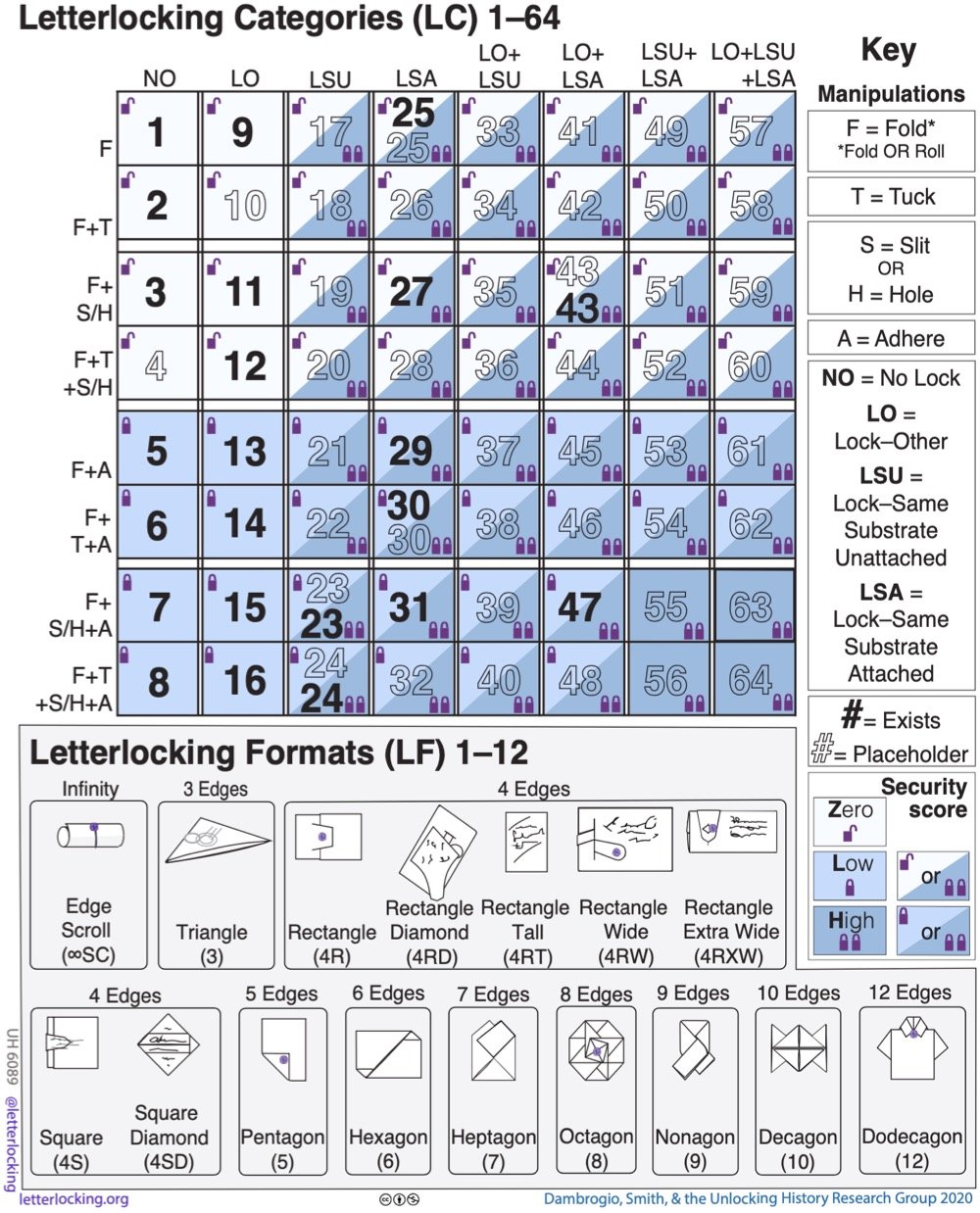
You can explore more about letterlocking at Letterlocking.org.
Update: The group investigating letterlocking is back in the NY Times with updated research.
Zeynep Tufekci has written an important piece for The Atlantic on the mistakes that the media, public health officials, and the public keep making during the pandemic and how we can learn from them. A big one for me is how scientists & other public health officials and agencies communicate their knowledge to the public and how the media interprets and amplifies those messages.
Thus, on January 14, 2020, the WHO stated that there was “no clear evidence of human-to-human transmission.” It should have said, “There is increasing likelihood that human-to-human transmission is taking place, but we haven’t yet proven this, because we have no access to Wuhan, China.” (Cases were already popping up around the world at that point.) Acting as if there was human-to-human transmission during the early weeks of the pandemic would have been wise and preventive.
Later that spring, WHO officials stated that there was “currently no evidence that people who have recovered from COVID-19 and have antibodies are protected from a second infection,” producing many articles laden with panic and despair. Instead, it should have said: “We expect the immune system to function against this virus, and to provide some immunity for some period of time, but it is still hard to know specifics because it is so early.”
Similarly, since the vaccines were announced, too many statements have emphasized that we don’t yet know if vaccines prevent transmission. Instead, public-health authorities should have said that we have many reasons to expect, and increasing amounts of data to suggest, that vaccines will blunt infectiousness, but that we’re waiting for additional data to be more precise about it. That’s been unfortunate, because while many, many things have gone wrong during this pandemic, the vaccines are one thing that has gone very, very right.
This pair of statements she highlights — “no clear evidence of human-to-human transmission” and “There is increasing likelihood that human-to-human transmission is taking place, but we haven’t yet proven this, because we have no access to Wuhan, China” — are both factually true but the second statement is so much more helpful, useful, and far less likely to be misinterpreted by people who aren’t scientists that making the first statement is almost negligent.
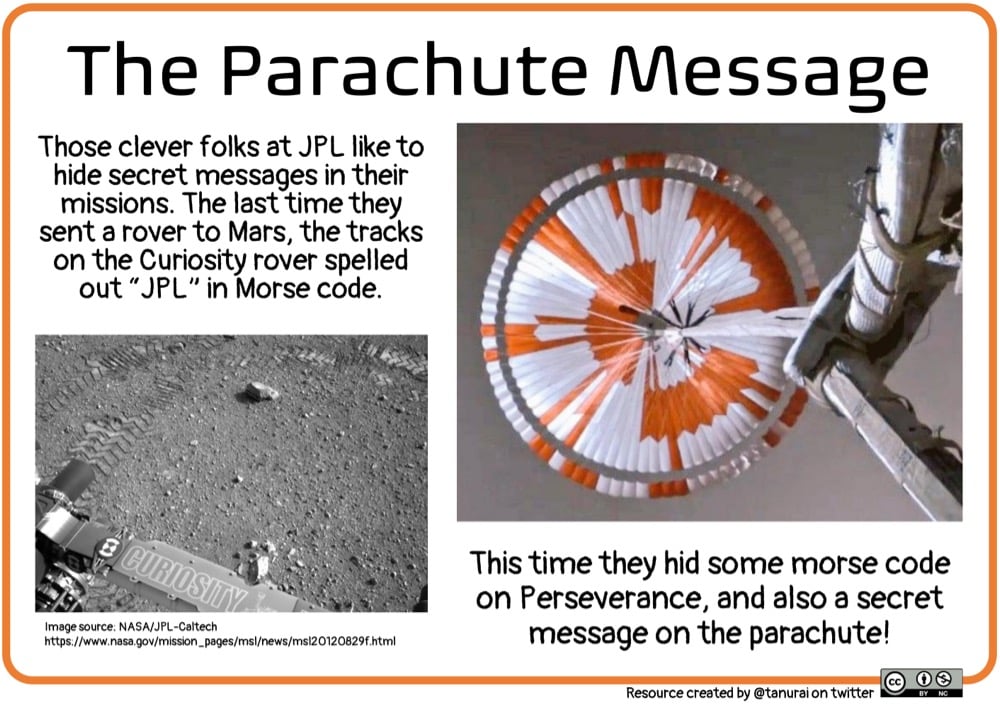
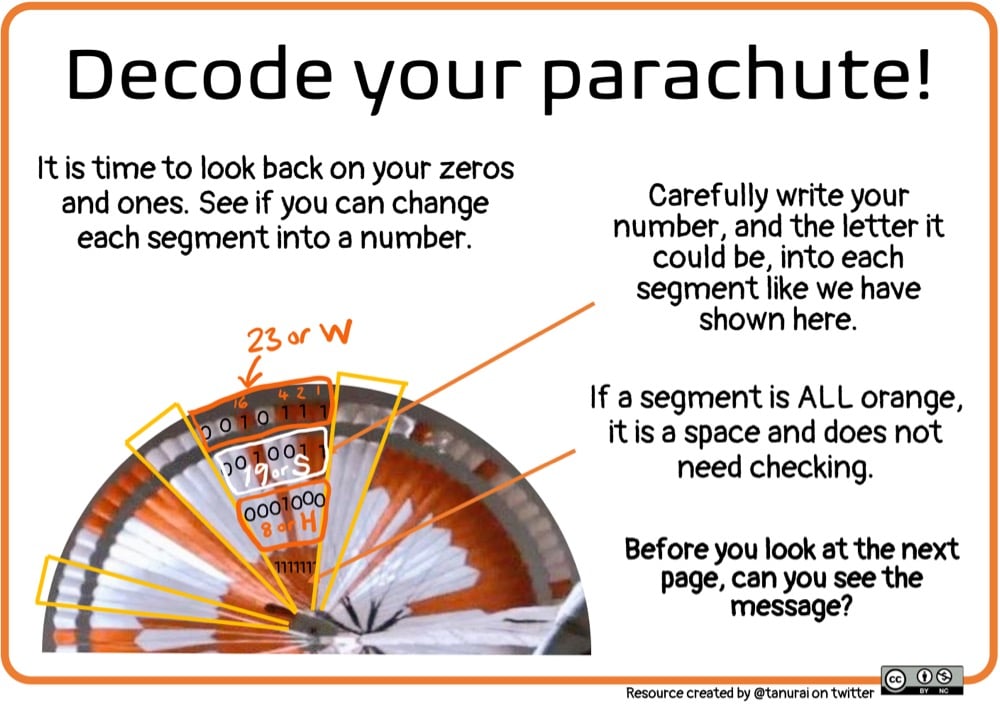
NASA engineers encoded a secret message in the parachute the Perseverance rover used to slow its descent to the surface of Mars. Tanya Fish provided a handy guide to decoding it on Twitter and as a PDF available on GitHub.
Just a few days after the Perseverance rover successfully touched down on Mars, NASA has released onboard video from the descent and landing from multiple perspectives. I watched this with my kids last night and all three of us had our mouths hanging open.
The real footage in this video was captured by several cameras that are part of the rover’s entry, descent, and landing suite. The views include a camera looking down from the spacecraft’s descent stage (a kind of rocket-powered jet pack that helps fly the rover to its landing site), a camera on the rover looking up at the descent stage, a camera on the top of the aeroshell (a capsule protecting the rover) looking up at that parachute, and a camera on the bottom of the rover looking down at the Martian surface.
After watching it again just now, I am struck by two things:
- Sometime in my lifetime, live broadcasts from Mars will likely become commonplace. There will be dozens or hundreds of Mars webcams you can pull up on whatever the 2052 internet equivalent is. It will be amazing how boring it all is. (Or perhaps it’ll be boring how amazing it all is.)
- That humans landed on the Moon in 1969 was an incredible feat, but a close second is that the first steps were broadcast live from the Moon’s surface to everywhere on the Earth. Unbelievable.
Can’t wait to see more from Perseverance once the science program gets cranking.
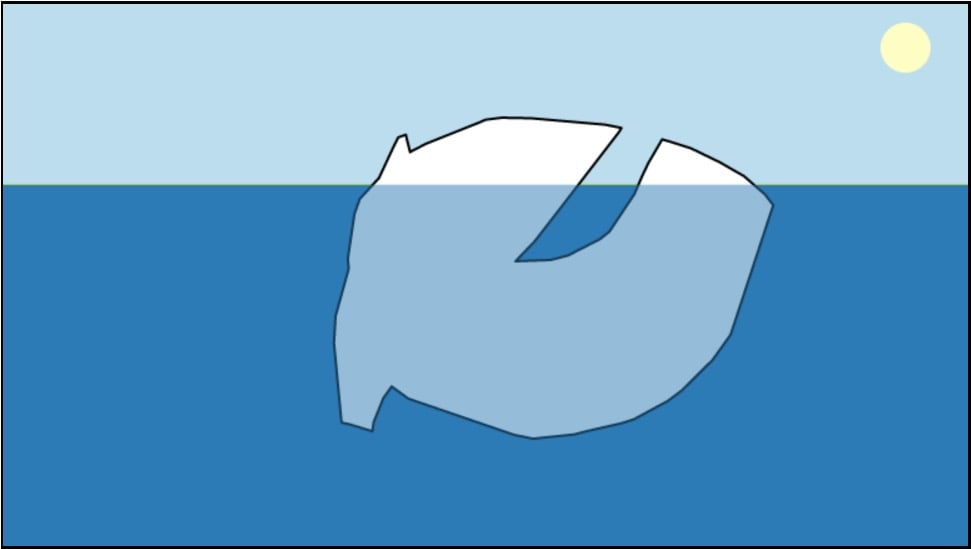
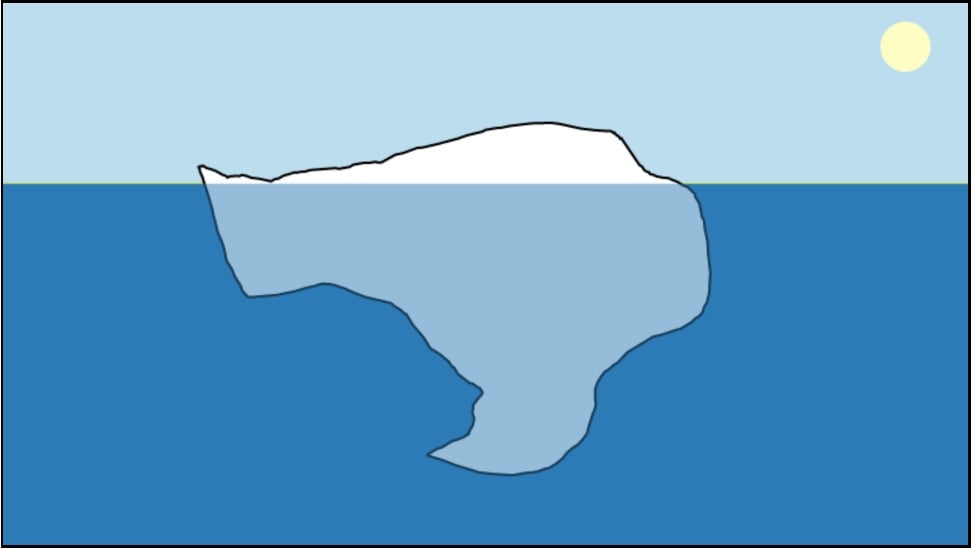
Glaciologist Megan Thompson-Munson recently posted an “unofficial but passionate petition” for scientists and science publications to start drawing icebergs correctly.
While it’s true that only ~10% floats above the surface of the water, the “classic” orientation is unstable and would actually not be found in nature. An elongated iceberg would not float on its head, but instead on its side.
Inspired by her plea, Joshua Tauberer made a cool little iceberg simulator called Iceberger — you can quickly draw an iceberg and see how it will float. Here are a couple of weird ones I drew:
I would love to see a gently gamified version of this where you compete to draw the slowest-orienting icebergs or icebergs closest to their stable orientation. Would be similar to some of the puzzles in Brain It On!
Update: See also Iceberger Remixed, an iceberg simulator with additional features.
Today is the day! NASA’s latest Mars rover is scheduled to touch down on the surface of Mars at around 3:55pm EST today1 and you can follow along online. You probably know the drill by now: what you’ll be watching isn’t actually live (it’s delayed by 11 minutes & 22 seconds, the time it takes for data to reach the Earth from Mars) and there’s no video to watch…there’s just telemetry from the rover that indicates where it is and what it’s doing. But I can say having watched the Curiosity landing in 2012, it’s still super exciting and nerve-wracking.
NASA has a number of ways to watch online, including their main stream on YouTube (embedded above), en Español, the “clean feed” from mission control without commentary, and a 360-degree stream, as well as options on Twitter, Facebook, Twitch, etc. You can also watch on NASA TV or through NASA apps on your phone, tablet, or TV. The coverage starts at 2:15pm EST (find your local time) and if all goes well, things start to get exciting at about 3:38pm EST and the landing will happen around 3:55pm EST. To get ready, you can check this page for a schedule of what happens when, watch a video about what’s gonna happen, and look at this live simulated view of where the Perseverance spacecraft is now (here too). Good luck, little rover!
In popular press and social media, there’s been a misunderstanding of what is actually meant when scientists say that the Pfizer and Moderna Covid-19 vaccines have an efficacy of 94-95%. It does not mean that 95% of vaccinated people are protected from infection — these vaccines are better than that. Dr. Piero Olliaro explains in a letter to The Lancet:
The mRNA-based Pfizer and Moderna vaccines were shown to have 94-95% efficacy in preventing symptomatic COVID-19, calculated as 100 x (1 minus the attack rate with vaccine divided by the attack rate with placebo). It means that in a population such as the one enrolled in the trials, with a cumulated COVID-19 attack rate over a period of 3 months of about 1% without a vaccine, we would expect roughly 0.05% of vaccinated people would get diseased.
Another way to put it: you’re 20 times less likely to get Covid-19 with a vaccine than without. (And again, data indicates these are safe vaccines.) Olliaro explains with some simple math:
If we vaccinated a population of 100,000 and protected 95% of them, that would leave 5000 individuals diseased over 3 months, which is almost the current overall COVID-19 case rate in the UK. Rather, a 95% vaccine efficacy means that instead of 1000 COVID-19 cases in a population of 100,000 without vaccine (from the placebo arm of the abovementioned trials, approximately 1% would be ill with COVID-19 and 99% would not) we would expect 50 cases (99.95% of the population is disease-free, at least for 3 months).
And of course if you vaccinate widely, it becomes a compounding situation because the virus just runs out of people to infect.
Over the past week or two, I’ve read a number of articles and threads about why Covid-19 cases are falling so rapidly in the US. The explanations have all been somewhat unsatisfying to me. Cases have indeed dropped off quite quickly and it happened pretty uniformly all over the country. Look at the mini state graphs on the NY Times Covid page — they all look about the same. Hospitalizations and positivity rates have dropped too, so while the number of daily tests has fallen too, this appears to be a real drop and not just an artifact of a lack of testing. Which is great news! Imagine a February and March that looked like December — a disaster compounded.
So what’s going on here? For The Atlantic, Derek Thompson lists four reasons for the decline in cases and hospitalizations that mirror the arguments I’ve seen elsewhere: “social distancing, seasonality, seroprevalence, and shots”.
The vaccine explanation is the weakest one for me: not enough people outside of healthcare workers had gotten them early enough to start bending that curve sharply downward in early January. But as Thompson notes, it could be having more of an effect on hospitalizations because the folks getting shots (and therefore immunity against severe infection) are those most likely to end up in hospitals due to infection. And obviously, vaccines are going to become the dominant factor in falling case numbers as more and more people get jabbed.
I’m also skeptical of the seasonality argument, but (again, as Thompson notes) there’s a lot we don’t know about how temperature, sunlight, humidity, and this specific coronavirus interact. Obviously Covid-19 is a seasonal thing and that’s definitely a contributing factor here, but that sharp of a drop in early January? I don’t know if it’s the primary driver here. Also, the seasonal flu typically peaks in February in the US.
The seroprevalence argument is an interesting one. Here’s Johns Hopkins infectious disease epidemiologist David Dowdy in a great Twitter thread about the US case decline:
I think the most logical explanation is one proposed initially by @mgmgomes1 and others — namely that we are seeing the effects of population immunity with heterogeneous mixing + strong behavioral effects. Take a(n overly) simple example. Assume 60% of a population has zero respiratory contacts, while the other 40% lives life as normal. If 75% of that high-mixing group has immunity (e.g., 30% population seroprevalence), you could easily see herd effects.
Basically, a large percentage of the folks at the greatest risk of getting Covid-19 in the US (i.e. folks who aren’t able or willing to keep from seeing other people and/or take proper precautions) have gotten it, resulting in a sort of localized “herd immunity” among those folks. After the massive holiday surge in cases (more on that in a sec), this hypothesis suggests, the virus started running out of people to infect and rates dropped quickly. This is the first explanation I read that really made sense to me.
Thompson leads off his piece with the behavioral explanation: “Maybe Americans finally got the hang of this mask and social-distancing thing.” I do not buy that people who previously weren’t doing so before suddenly started wearing masks (or better masks), keeping distant, spending less time indoors with others, and staying home from work started doing so in numbers large enough to cause such a sharp downturn. But you can’t consider the decline without also looking at how cases got so high in the first place. Here’s Steven Johnson on Twitter, zooming out a few months:
[It’s] not so much that people got the hang of social distancing, but rather that the holiday season compelled people to relax social distancing for in-person family gatherings. So the current decline is mostly reversion to where we were in Oct-Nov.
Yes, this. Without these holidays, we may have seen much more of a winter plateau than a spike. So here’s what seems plausible to me. As the cold weather made the coronavirus more effective at infection, people gathered for Halloween, Thanksgiving, Hanukkah, Christmas, and New Year’s — each subsequent holiday building on the previous one — and it pushed cases much higher than they would have been without those major gatherings. After two months of massive infection rates, the virus burned itself out among the high-mixing group and everyone else retreated back into their homes and pods to hunker down, resulting in the steep decline we’re seeing.
Obviously, careful scientific study will be necessary to tease out how significant each of these (and other!) causes were to the holiday spike and subsequent decline. But for now, the way forward is continuing to social distance, wear (better) masks, limit close contacts, and get people vaccinated — before B.1.1.7 and the other variants hit.
Curiosity is about to get some company. NASA’s newest rover, Perseverance, is set to land on Mars beginning tomorrow at around 3pm EST. The video above walks us through the 7-minute landing routine in which the rover ditches its spacecraft, heat shields its way through the Martian atmosphere, deploys its parachute, uses an onboard guidance system to navigate to a good landing spot, and finally is lowered down to the surface via a sky crane. The rover’s destination is Jezero Crater, site of an ancient river delta and lakebed.
Jezero Crater tells a story of the on-again, off-again nature of the wet past of Mars. More than 3.5 billion years ago, river channels spilled over the crater wall and created a lake. Scientists see evidence that water carried clay minerals from the surrounding area into the crater lake. Conceivably, microbial life could have lived in Jezero during one or more of these wet times. If so, signs of their remains might be found in lakebed or shoreline sediments. Scientists will study how the region formed and evolved, seek signs of past life, and collect samples of Mars rock and soil that might preserve these signs.
Here’s how you can watch the landing “live” tomorrow (i.e. delayed by the 11 minutes & 22 seconds it takes for signals to travel from Mars). I’ll do a separate post tomorrow w/ the proper YouTube embeds so we can all follow along together.

After 1405 nights of observation over 6 years, astronomers at three observatories have produced an image of the night sky that contains 10 trillion pixels of data and depicts over a billion galaxies. Bad Astronomy’s Phil Plait has the details.
It’s the result of the DESI Legacy Imagining Surveys, maps of the sky made by the three observatories (the Dark Energy Camera Legacy Survey, the Beijing-Arizona Sky Survey, and the Mayall z-band Legacy Survey, in combination with the orbiting WISE infrared observatory). They mapped the northern sky in seven colors, covering a third of the entire sky — 14,000 square degrees, or the equivalent area of 70,000 full Moons on the sky.
The ultimate goal is to better understand dark energy, the mysterious substance that’s accelerating the expansion of the Universe, by looking at the distribution of galaxies throughout the Universe. They’ll do that by picking tens of millions of the billion galaxies in the data and getting follow-up observations with the Dark Energy Spectroscopic Instrument (DESI), which will take spectra of those galaxies and find their distances.
Since we’ll know their positions on the sky, and their distances, this will make a 3D map of the Universe larger than any ever before.
The photo included at the top of the post is just a tiny tiny bit of the full image — you can pan and zoom the whole thing in this viewer. Be sure to zoom out in increments from the default view so as to fully appreciate just how absurdly large this image (and the universe) is.
In 1959, a group of students died while on a hiking trip in the Ural Mountains. The circumstances of the incident and the way in which they died presented a mystery that has remained unsolved in the decades since.
The Dyatlov Pass incident is an intriguing unsolved mystery from the last century. In February 1959, a group of nine experienced Russian mountaineers perished during a difficult expedition in the northern Urals. A snow avalanche hypothesis was proposed, among other theories, but was found to be inconsistent with the evidence of a lower-than-usual slope angle, scarcity of avalanche signs, uncertainties about the trigger mechanism, and abnormal injuries of the victims.
Now, researchers have come up with a plausible explanation of the accident: a low-angle avalanche enabled by unusually slippery snow and high winds. From a piece in Wired about the investigation:
The cross-country skiers had actually pitched camp on a small step in the hillside, scooping away the snow to level it out. When they cut into the snowpack, they sliced through the weak layer, essentially initiating a countdown. “When you create a cut in the slope to install the tent, it’s like when you remove a retaining wall,” says Gaume, a snow physicist at the Swiss Federal Institute of Technology. The slab of denser snow now hung precariously over the camp. “All the ingredients were there,” Gaume adds. “There was a weak layer, there was a slab, and the slope angle was locally steeper than the critical angle.”
Also from the Wired piece: the researchers were inspired by the realistic snow modeling that Disney did for Frozen. (via kottke ride home)
This guide to Covid-19 variants (SARS-CoV-2 viruses that have evolved changes to meaningfully alter their behavior) by Michaeleen Doucleff and Meredith Rizzo at NPR cleverly visualizes how mutations of the virus’s spike proteins help bind it more easily to ACE2 receptors on human cells. The key to the visualization is Meredith Miotke’s illustrations of the viruses using Lego pieces to represent the virus spikes and cell receptors. The usual SARS-CoV-2 has 1x1 Lego pieces that can bind with 1x2 pieces, like so:
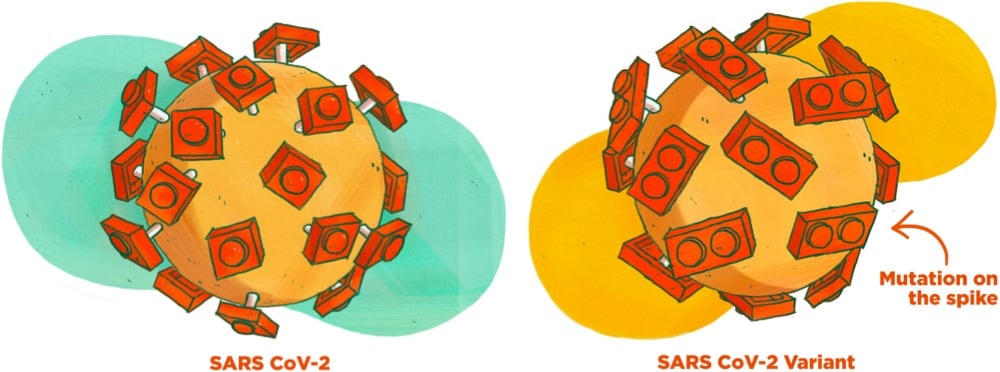
But, as everyone who has ever worked with a Lego set knows, a 1x1 piece stuck to a 1x2 piece is not super stable. So when a version of the virus with a 1x2 piece shows up, it’s able to form a better connection to the 1x2 receptor:
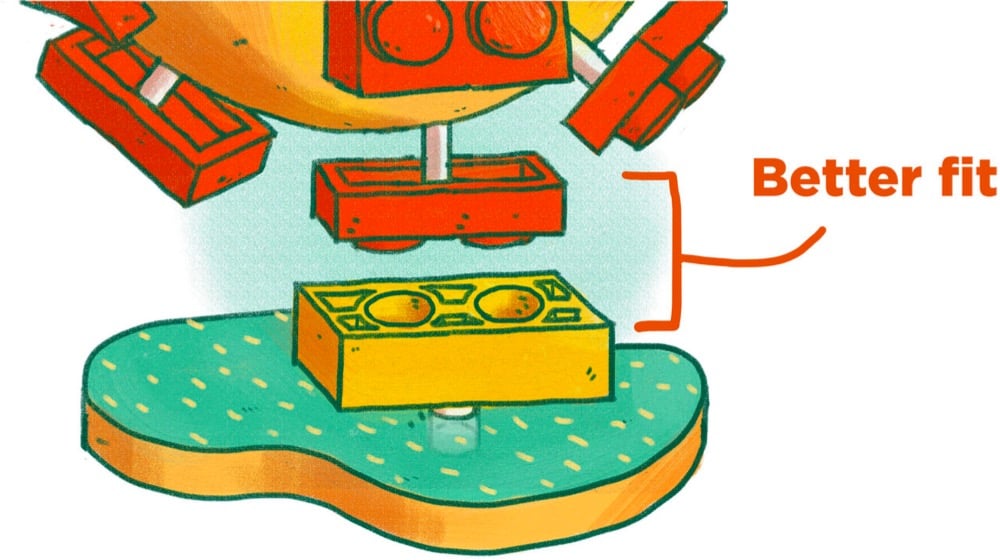
The analogy breaks down if you look too hard at it1 but for many people, it can be a quick way to get the gist of the mechanism at work here. (via @EricTopol)
Using images from the Kaguya orbiter, Seán Doran has constructed a 4-hour realtime orbit of the Moon. Feel free to pair with your favorite piece of relaxing music for a meditative viewing experience.
See also another video by Doran: An Incredible Video of What It’s Like to Orbit the Earth for 90 Minutes.

You probably read something yesterday, maybe just a headline, about Moderna’s Covid-19 vaccine being “six times less effective” against the B.1.351 coronavirus variant first identified in South Africa. This is, to put it plainly, a bullshit take on what is actually excellent news. This is the important bit, via Stat:
Both the Moderna vaccine and the immunization from Pfizer-BioNTech produce such powerful levels of immune protection — generating higher levels of antibodies on average than people who recover from a Covid-19 infection have — that they should be able to withstand some drop in their potency without really losing their ability to guard people from getting sick.
“There is a very slight, modest diminution in the efficacy of a vaccine against it, but there’s enough cushion with the vaccines that we have that we still consider them to be effective,” Anthony Fauci, the top U.S. infectious diseases official, said Monday on the “Today” show.
Let’s hear that again: “Both the Moderna vaccine and the immunization from Pfizer-BioNTech produce such powerful levels of immune protection…” These vaccines are so good, so potent, that even this sixfold drop in one measure of the vaccines’ ability to neutralize this one SARS-CoV-2 variant isn’t even enough to significantly reduce their overall protective power.1 That’s the important news here, that’s the very good news, that’s what you should be taking away from this. We have miraculously developed a near-perfect medicine for a plague that has significantly disrupted all human life on Earth and we’re flipping out over some technical details that the experts assure us don’t mean much in terms of overall effectiveness?! No thank you. Not today.
In a Twitter thread, Zeynep Tufekci is tearing her hair out because of the media’s misunderstanding and sensationalization of the “sixfold drop”.
I know people are tired but needless anxiety isn’t helping us. Let’s focus on getting through these months — better masks if indoors with others, more strict attention to our precautions — and the real problem: making more of these amazing vaccines quickly & getting them out there!
I get it, we want to understand but not how it works. Stop worrying about Nab titers. That does NOT mean the vaccine is six times less effective. People whose job it is to worry about it are on it & we just got confirmation: it works against the variants.
Plea to media: this isn’t a good headline. It makes people think the vaccine is six times less effective against the new variants (FALSE!) when the news today is *excellent*: The vaccine continues to work well against the new variants. That’s the headline.
For a much more technical take on the efficacy of the vaccines against variants, see virologist Florian Krammer’s long thread. His conclusion:
mRNA vaccines induce very high neutralizing antibodies after the second shot (consistently in the upper 25-30% of what we see with convalescent sera). If that activity is reduced by 10-fold, it is still decent neutralizing activity that will very likely protect. Furthermore, we know that the mRNA vaccines are already protective after the first shot when neutralizing antibody titers are low or undetectable in most individuals.
There is a concern here and it’s that B.1.351 or B.1.1.7 might mutate into variants that are significantly resistant against the vaccines’ good effects. Krammer again:
First, we need to do what every good scientist is praying for a year now: We need to cut down on virus circulation. The more the virus replicates, the more infections there are the higher are the chances for new variants to arise. Also, we need to try and contain B.1.351 and B.1.1.248/P.1 as much as possible.
That’s why, aside from preventing hundreds of thousands of deaths in the next several months, getting these vaccines into people’s arms is so important: the less the virus spreads, the less opportunity it will have to mutate into something even more dangerous. The US vaccination effort is slowly ramping up — we’re at an average of 1.3 million doses per day right now and the trend is heading in the right direction. We can get this done!
So what can you do about this right now? 1. Stop worrying about the variants until the experts let us know we have something to worry about. 2. If you are eligible for the vaccine, get it! 3. Spread the word about vaccine availability in your area. Yesterday Vermont opened signups for vaccination appointments for all Vermonters 75 and older, and I texted/emailed everyone I could think of who was over 75 or who had parents/relatives/friends who are over 75 to urge them to sign up or spread the word. 4. Continue to wear a mask (a better one if possible), wash your hands, social distance, stay home when possible, don’t spend time indoors w/ strangers, etc. Thanks to these remarkable vaccines, real relief is in sight — let’s keep on track and see this thing through.
In response to comments about a video of him getting the Covid-19 vaccine — “Come with me if you want to live!” — Arnold Schwarzenegger says that if you want to build biceps, you should listen to him. He’s the expert. But if you want to know what to do about Covid-19, you should listen to epidemiologists and doctors.
Dr. Fauci and all of the virologists and epidemiologists and doctors have studied diseases and vaccines for their entire lives, so I listen to them and I urge you to do the same. None of us are going to learn more than them by watching a few hours of videos. It’s simple: if your house is on fire, you don’t go on YouTube, you call the damn fire department. If you have a heart attack, you don’t check your Facebook group, you call an ambulance. If 9 doctors tell you you have cancer and need to treat it or you will die, and 1 doctor says the cancer will disappear, you should always side with the 9. In this case, virtually all of the real experts around the world are telling us the vaccine is safe and some people on Facebook are saying it isn’t.
In general, I think if the circle of people you trust gets smaller and smaller and you find yourself more and more isolated, it should be a warning sign that you’re going down a rabbit hole of misinformation. Some people say it is weak to listen to experts. That’s bogus. It takes strength to admit you don’t know everything. Weakness is thinking you don’t need expert advice and only listening to sources that confirm what you want to believe.


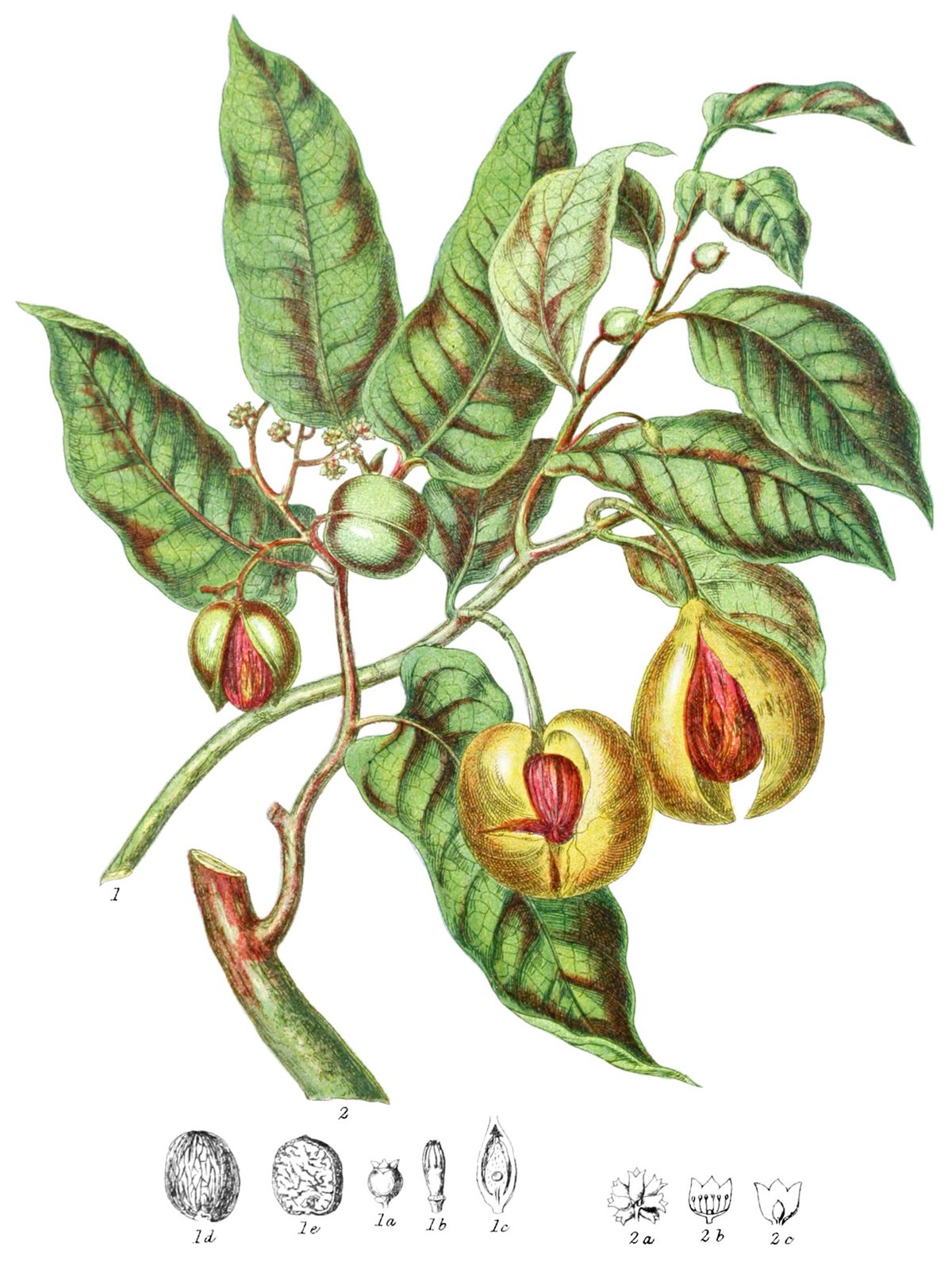
Nicholas Rougeux has beautifully reproduced & remastered botanical illustrator Elizabeth Twining’s catalog of plants and flowers from 1868, Illustrations of the Natural Orders of Plants. Each of the 160 illustrations is accompanied by explanatory text from the original book and an interactive version of the image (click on the highlighted plant for more info).
Posters based on the illustrations are available and, get this, so are puzzles!
In an opinion piece for the NY Times, Zeynep Tufekci and epidemiologist Michael Mina are urging for new trials of the Moderna and Pfizer/BioNTech Covid-19 vaccines to begin immediately to see how effective a single dose might be in preventing new infections. If the trials do indicate that a single dose works, that would effectively double the number of people we could vaccinate within a certain time period, saving countless lives in the US and worldwide.
Both vaccines are supposed to be administered in two doses, a prime and a booster, 21 days apart for Pfizer and 28 days for Moderna. However, in data provided to the F.D.A., there are clues for a tantalizing possibility: that even a single dose may provide significant levels of protection against the disease.
If that’s shown to be the case, this would be a game changer, allowing us to vaccinate up to twice the number of people and greatly alleviating the suffering not just in the United States, but also in countries where vaccine shortages may take years to resolve.
But to get there — to test this possibility — we must act fast and must quickly acquire more data.
For both vaccines, the sharp drop in disease in the vaccinated group started about 10 to 14 days after the first dose, before receiving the second. Moderna reported the initial dose to be 92.1 percent efficacious in preventing Covid-19 starting two weeks after the initial shot, when the immune system effects from the vaccine kick in, before the second injection on the 28th day
That raises the question of whether we should already be administrating only a single dose. But while the data is suggestive, it is also limited; important questions remain, and approval would require high standards and more trials.
The piece concludes: “The possibility of adding hundreds of millions to those who can be vaccinated immediately in the coming year is not something to be dismissed.”
If you crack a fertilized chicken egg into a transparent container — in this case, plain old kitchen plastic wrap — and incubate it, you can observe the embryo as it develops and eventually “hatches” into a chick, heartbeat and all. The process takes about 21 days from start to finish.
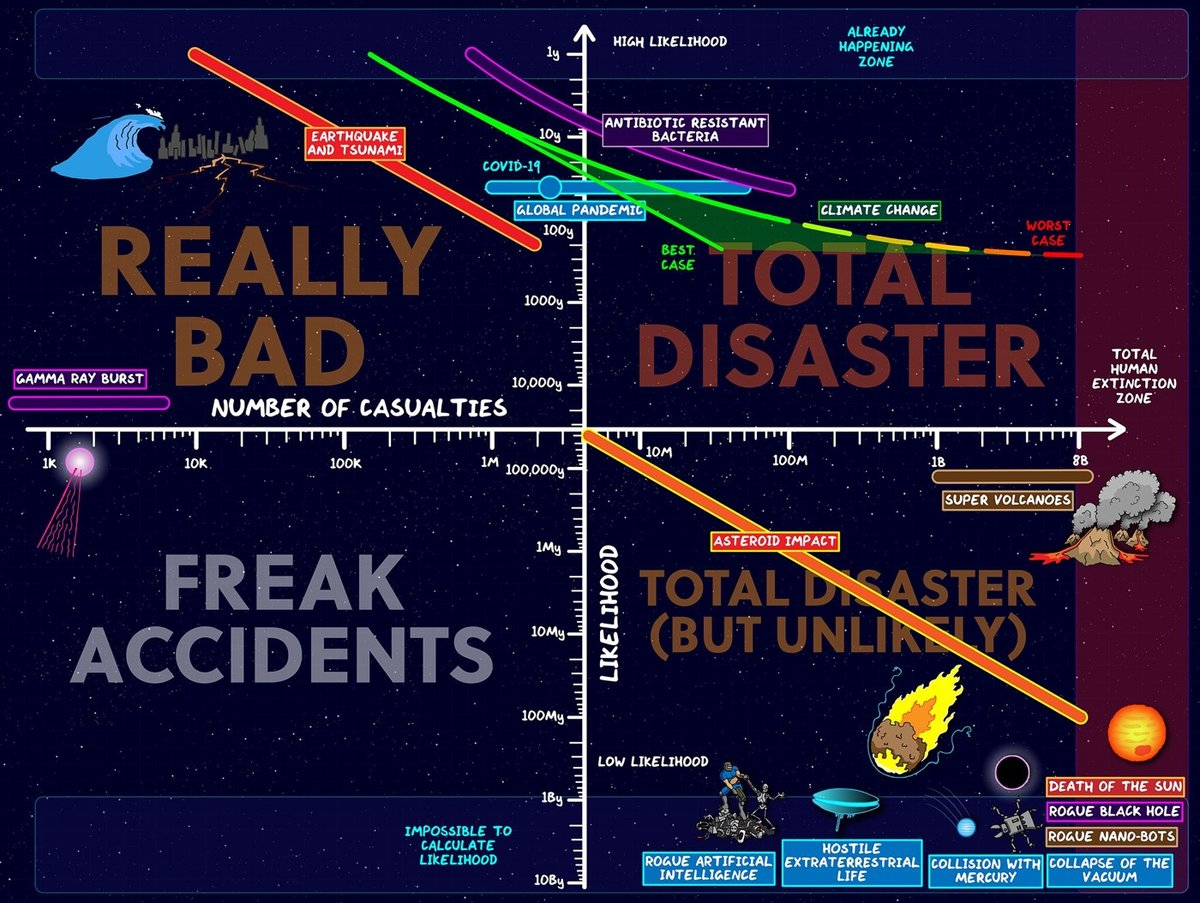
Spurred by the pandemic — what he calls “the first experience we’ve had of a global disaster affecting every single person on Earth”1 — Domain of Science’s Dominic Walliman takes stock of many of the possible catastrophes that might befall humanity, ranking possible threats based on their likelihood and the number of potential casualties.
This year was the first experience we’ve had of a global disaster affecting every single person on Earth. And also how unprepared society was to deal with it, despite plenty of people giving warnings that this was going to happen at some stage.
But in the midst of all the doom I started to wonder, what other things could threaten humanity, that we are not thinking about? So I made the Map of Doom to list all the threats to humanity in one place.
The result is the quadrant chart and the video above as well as the Map of Doom.
One could imagine a third dimension of this chart: what, if anything, humans can do about each of these threats. Earthquakes can be detected, buildings can be designed to withstand them, and evacuation procedures enacted and prioritized. Many effects of climate change can be mitigated. Asteroids can be detected, but doing something about them might prove difficult. We’ve lowered the threat of nuclear war — for now. Supervolcanoes? Yikes.
You can find a list of references used in the video’s description. (via open culture)
In remarks to the German parliament today, German Chancellor Angela Merkel advocated for tighter Covid-19 restrictions, as cases & deaths in Germany reach new peaks. The restrictions she’s referring to were recommended by “a national academy of scientists and academics” and are intended at reducing the spread of Covid-19 over the December holidays. The impassioned argument that she makes in this short video clip (full report here) is difficult for me to find fault with (even though conservative members of her parliament and Twitter commenters disagree). Here’s a partial transcript:
If the price we pay is 590 deaths per day, then that is unacceptable in my view. And when scientists are practically begging us to reduce our contacts for a week before we see Grandma and Grandpa, grandparents and older people at Christmas, then perhaps we really should think again about whether we can’t find a way to start the school holidays on the 16th instead of the 19th. What will we say when we look back on this once-in-a-century event if we weren’t able to find a solution for these three days? And it may be the case that sending children home is the wrong thing to do, if so then it will have to be digital lessons or something else. I don’t know, this is not my area of expertise and I don’t want to interfere. I only want to say: if we have too many contacts now, in the run-up to Christmas, and it ends up being the last Christmas with our grandparents, then we will have done something wrong. She should not let this happen.
I teared up watching her talk. In the US, we are dealing with many more cases (which will turn into eventual deaths) and deaths than Germany, both in absolute and per capita terms. It’s like 10 fully-loaded passenger planes a day are crashing with no survivors and there are small things that we all can do to keep many of those people alive and … many of us just don’t want to do those things!
Like Merkel says, we are going to look back on this and be completely ashamed that we didn’t do these things and that we elected people that won’t advocate for these things on our behalf and that we let 300-400,000 Americans die and countless others lose loved ones and go bankrupt and get evicted and lose their businesses and be chronically ill and be food insecure and and and. If we aren’t ashamed, if we don’t reckon with all of this someday, then maybe nothing can redeem us and we deserved it all.
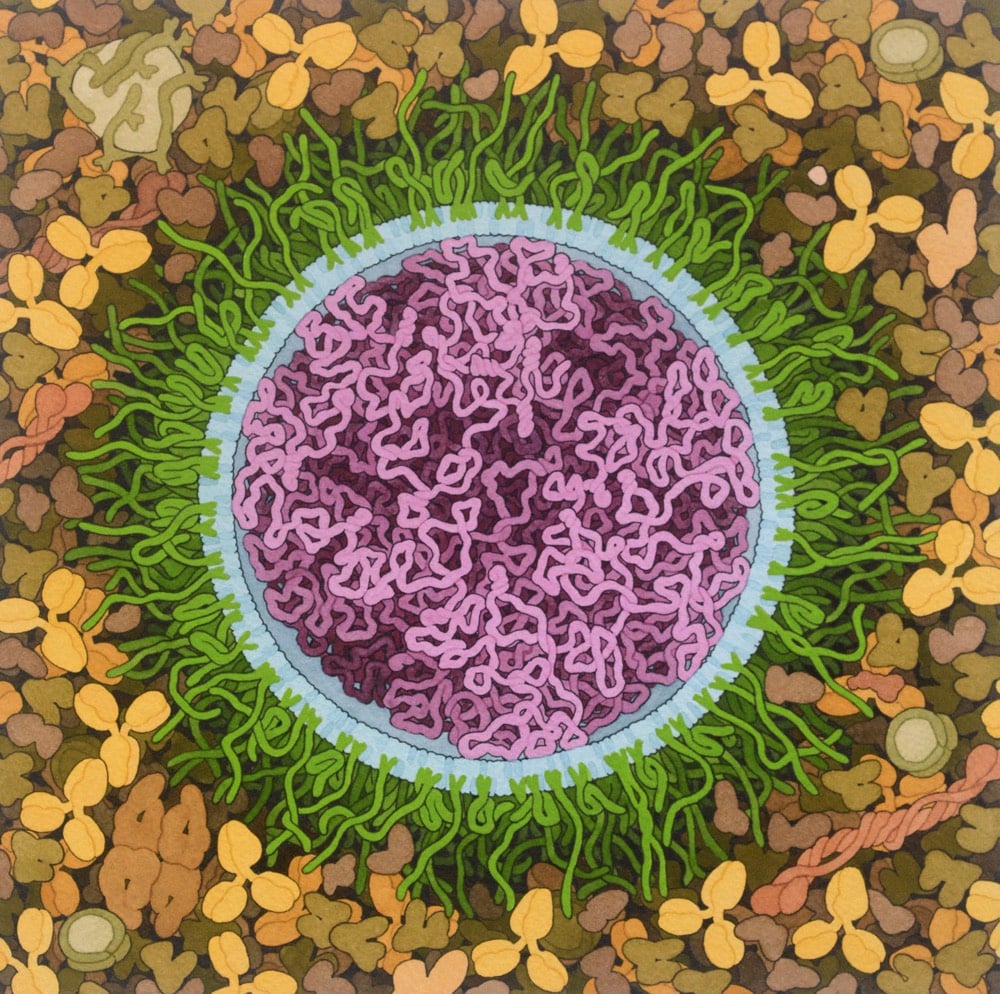
Artist and biologist David Goodsell has done a painting of the Covid-19 mRNA vaccine.
The vaccine structure is highly idealized, with spike mRNA in magenta, lipids in blue, and PEG-lipid in green. The background is blood serum or lymph.
Both the Pfizer/BioNTech and the Moderna Covid-19 vaccines are based on mRNA — you can brush up on how they work at Stat or the CDC.
mRNA vaccines are a new type of vaccine to protect against infectious diseases. To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, they teach our cells how to make a protein — or even just a piece of a protein — that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.
See also Goodsell’s painting of a SARS coronavirus from back in February.
The NY Times recently surveyed 700 epidemiologists about how they are personally living during the pandemic and what they think is going to happen next. Epidemiologists should have a better idea than most of us about how to act during a viral pandemic, so there’s lots of good information in there about vaccines and high-risk behaviors. But I found their answers to a pair of speculative questions about a return to normalcy most interesting.
How and when will life go back to normal?
“For some, it has gone back to normal, and because of this, it will be two to three years before things are back to normal for the cautious, at least in the U.S.”
- Cathryn Bock, associate professor, Wayne State University
“The new normal will be continued masking for the next 12 to 18 months and possibly the next few years. This is a paradigm shift.”
- Roberta Bruhn, co-director, Vitalant Research Institute
What will never return to normal?
“My relationships with people who have taken this pandemic lightly and ignored public health messages and recommendations.”
- Victoria Holt, professor emeritus, University of Washington
“Every part of my daily life that involves interaction with anyone other than my spouse.”
- Charles Poole, associate professor, University of North Carolina
For many people, the pandemic has altered almost every aspect of their lives. If we listen to what epidemiologists are telling us (like we should have back in early 2020 to avoid much of our present hardship), it could help us accept that the pandemic will continue to affect most aspects of our lives even after it is “over”.
Free Covid-19 illustration courtesy of Pixel True.
Zeynep Tufekci reports on a small study from Korea that has big implications on how we think about transmission of SARS-CoV-2. Scientists traced two cases back to a restaurant and discovered that transmission had occurred over quite a long distance in a very short period of time.
If you just want the results: one person (Case B) infected two other people (case A and C) from a distance away of 6.5 meters (~21 feet) and 4.8m (~15 feet). Case B and case A overlapped for just five minutes at quite a distance away. These people were well beyond the current 6 feet / 2 meter guidelines of CDC and much further than the current 3 feet / one meter distance advocated by the WHO. And they still transmitted the virus.
As Tufekci goes on to explain, the way they figured this out was quite clever: they contact traced, used CCTV footage from the restaurant, recreated the airflow in the space, and verified the transmission chain with genome sequencing. Here’s a seating diagram that shows the airflow in relation to where everyone was sitting:
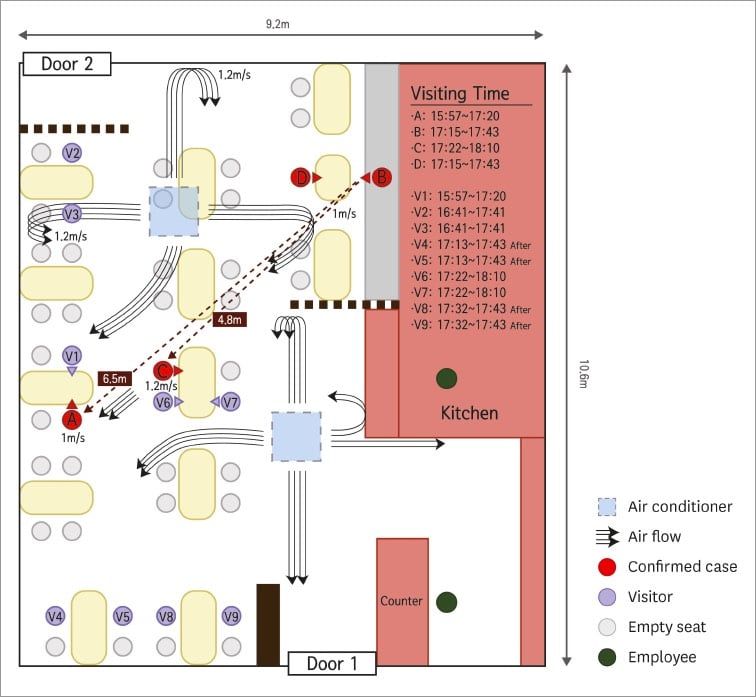
Someone infecting another person 21 feet away in only five minutes while others who were closer for longer went uninfected is an extraordinary claim and they absolutely nailed it down. As Sherlock Holmes said: “Once you eliminate the impossible, whatever remains, no matter how improbable, must be the truth.” And the truth is that in some cases, the recommended 6 feet of distance indoors is not sufficient when people aren’t wearing masks. Airflow matters. Ventilation matters. Which way people are facing matters. How much people are talking/laughing/yelling/singing matters. Masks matter. 6 feet of distance does not confer magical protection. All that can make it tough to figure out if certain situations are safe or not, but for me it’s an easy calculation: absolutely no time indoors with other people not wearing masks. Period. As Tufekci concludes:
I think there are three broad lessons here. One, small data can be extremely illuminating. Two, air flow and talking seem to matter a great deal. Three, sadly, indoor dining and any activity where people are either singing or huffing and puffing (like a gym) indoors, especially with poor ventilation, clearly remains high risk.
Read her whole post — as she says, it’s “perhaps one of the finest examples of shoe-leather epidemiology I’ve seen since the beginning of the pandemic”.
The Milky Way galaxy may be home to billions or even trillions of rogue planets (planets that don’t orbit stars). In this video, Kurzgesagt considers how the Earth could go rogue (by following a nearby massive star away from the Sun) and what would happen to our oceans, atmosphere, and lives if it happened.
The first part of the video is pretty bleak — “as the days turn dark, the final winter of humanity would begin” — while the second part is hopeful: we’ll be able to predict our ejection thousands of years before it happens and may be able to prepare. In light of the world’s response to the pandemic and climate change, it would certainly be interesting to see if human civilization could get it together to save itself from a cold death in outer space. I have no doubt that scientist could accurately diagnose the problem and supply solutions, but the politics would be a total mess.
With the first approved Covid-19 vaccines set to roll out in the US soon, some of the focus has shifted to how the vaccine will be distributed and its equitable allocation. Part of the distribution logistics puzzle is making sure there are enough glass vials to hold and transport the vaccine around the nation to those waiting to be vaccinated. For the New Yorker, Christopher Payne took some photos of two Corning factories that are manufacturing vials as fast as they can.
But back in the early 19th century, for a colonial empire dealing with overseas smallpox epidemics, glass vials were not an option. Smallpox vaccination at that time was most reliably accomplished by transferring material from cowpox blisters on one person (or cow) to another person. The freshly inoculated person got a little sick but later proved to be immune to the much deadlier smallpox. So when Spain’s Royal Philanthropic Vaccine Expedition set sail in 1803 to inoculate the inhabitants of their overseas colonies for smallpox, they used the bodies of human beings to transport the vaccine. To be more specific, they used “twenty-two orphan boys, ages three to nine”.1
And so it was that, “in the era before refrigeration, freeze-dried vaccines, and jet aircraft,” writes medical historian John Bowers, “the successful circumnavigation of the globe with the vaccine…rested on a single medium — little boys.” During the long crossing, approximately twenty-two orphans who had not previously contracted smallpox or cowpox were “vaccinated in pairs every ninth or tenth day,” via arm-to-arm inoculation (taking lymph from an unbroken pustule on a recently vaccinated boy and introducing it under the skin of another). This created a vaccine chain — the vaccine remained active and viable for the entire journey.
The three-year expedition was success and an early & effective example of philanthropic healthcare, but you also have to note here that the reason the Americas were ravaged by smallpox was because Spain brought it there in the first place.
Update: In The Atlantic, Sam Kean provides some more detail on the vaccination effort.
Given the era, it’s likely that no one asked the orphans whether they wanted to participate — and some seemed too young to consent anyway. They’d been abandoned by their parents, were living in institutions, and had no power to resist. But the Spanish king, Carlos IV, decided to make them a few promises: They would be stuffed with food on the voyage over to make sure they looked hearty and hale upon arrival. After all, no one would want lymph from the arm of a sickly child. Appearance mattered. And they’d get a free education in the colonies, plus the chance at a new life there with an adoptive family. It was a far better shake than they’d get in Spain.
Newer posts
Older posts
Socials & More