kottke.org posts about science
The CDC recently released their report on Mortality in the United States, 2020 and this graph of US life expectancy at birth since 1950 by Christopher Ingraham dramatically summarizes the report’s main finding:
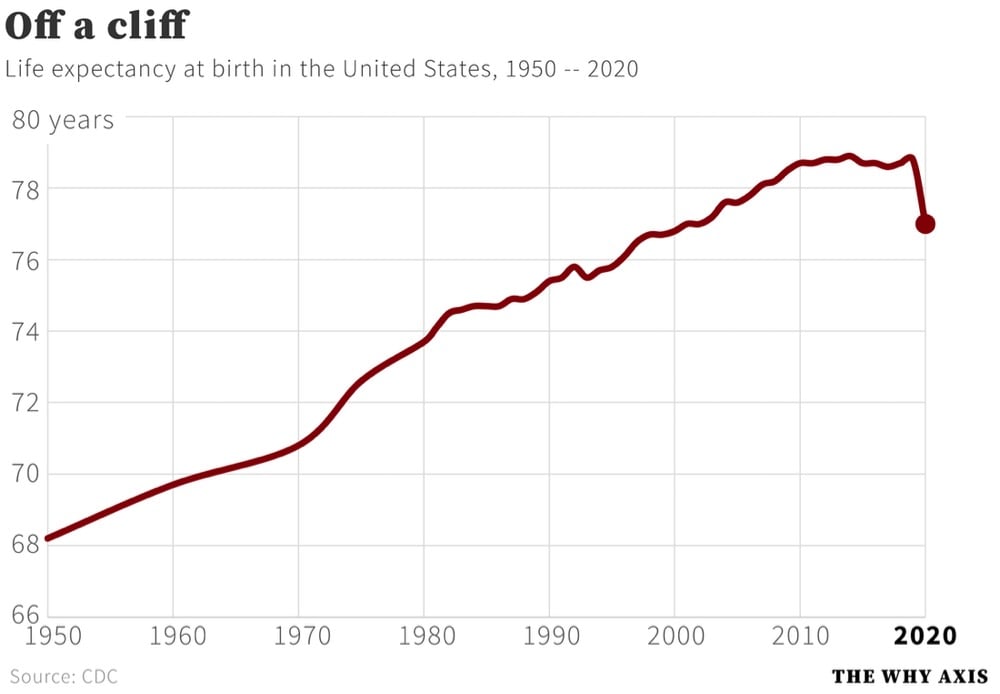
That’s a decrease in life expectancy of 1.8 years from 2019. Here are some more of the report’s significant findings:
In 2020, life expectancy at birth was 77.0 years for the total U.S. population — a decrease of 1.8 years from 78.8 years in 2019. For males, life expectancy decreased 2.1 years from 76.3 in 2019 to 74.2 in 2020. For females, life expectancy decreased 1.5 years from 81.4 in 2019 to 79.9 in 2020.
In 2020, the difference in life expectancy between females and males was 5.7 years, an increase of 0.6 year from 2019.
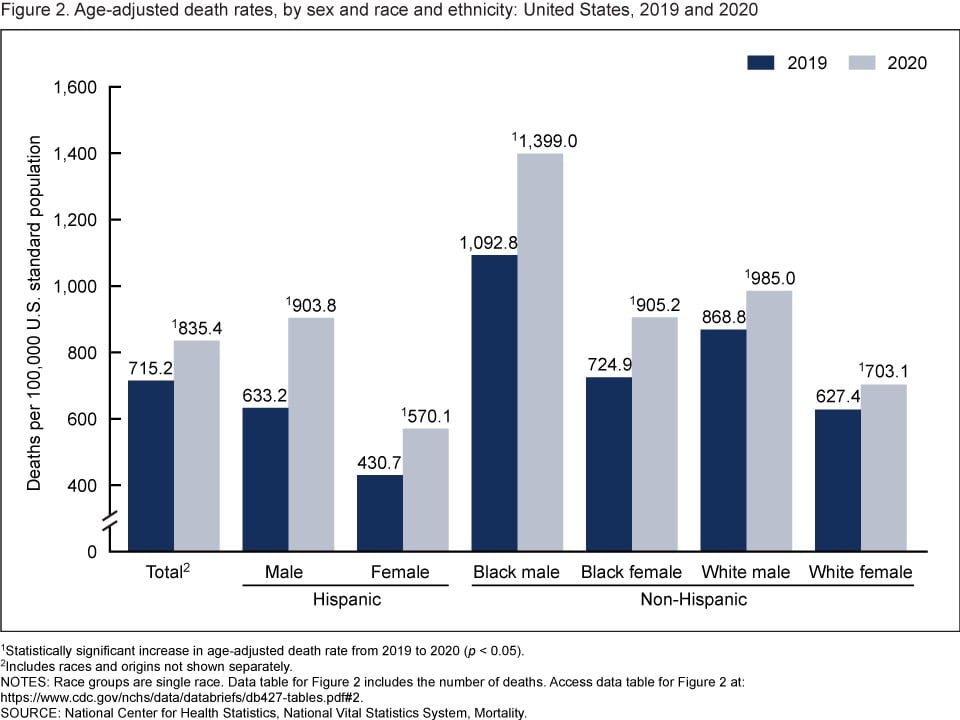
The age-adjusted death rate for the total population increased 16.8% from 715.2 per 100,000 standard population in 2019 to 835.4 in 2020. Age-adjusted death rates increased in 2020 from 2019 for all race-ethnicity-sex groups, increasing 42.7% for Hispanic males, 32.4% for Hispanic females, 28.0% for non-Hispanic Black males, 24.9% for non-Hispanic Black females, 13.4% for non-Hispanic White males, and 12.1% for non-Hispanic White females.
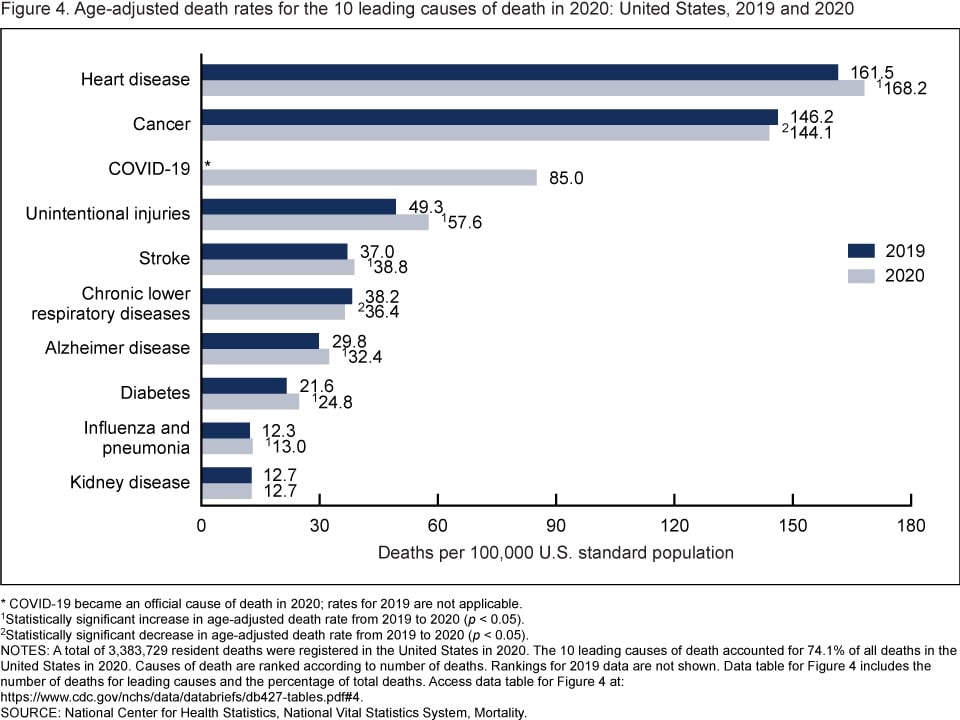
In 2020, 9 of the 10 leading causes of death remained the same as in 2019. The top leading cause was heart disease, followed by cancer. COVID-19, newly added as a cause of death in 2020, became the 3rd leading cause of death. Of the remaining leading causes in 2020 (unintentional injuries, stroke, chronic lower respiratory diseases, Alzheimer disease, diabetes, influenza and pneumonia, and kidney disease), 5 causes changed ranks from 2019. Unintentional injuries, the 3rd leading cause in 2019, became the 4th leading cause in 2020. Chronic lower respiratory diseases, the 4th leading cause in 2019, became the 6th. Alzheimer disease, the 6th leading cause in 2019, became the 7th. Diabetes, the 7th leading cause in 2019, became the 8th. Kidney disease, the 8th leading cause in 2019, became the 10th leading cause in 2020. Stroke, and influenza and pneumonia, remained the 5th and 9th leading causes, respectively. Suicide dropped from the list of 10 leading causes in 2020.
And from the report’s summary:
From 2019 to 2020, the age-adjusted death rate for the total population increased 16.8%. This single-year increase is the largest since the first year that annual mortality data for the entire United States became available. The decrease in life expectancy for the total population of 1.8 years from 2019 to 2020 is the largest single-year decrease in more than 75 years.
Since more people in the US died of Covid in 2021 than in 2020, I’d expect the decline life expectancy and the rise in death rate to continue.
In the mid-1820s, the naturalist Charles Darwin began his research career studying botany in university and he bought a portable brass microscope to aid him in his studies. The microscope was passed down through the generations of his family and was recently sold at auction for ~$790,000.
Charles Darwin’s own research career began in earnest with the more prosaic, but no less philosophical, investigation into the sea creatures being dredged up from the Firth of Forth, which Charles obtained from friendly fishermen while he was trying to avoid his medical studies at the University of Edinburgh. Darwin’s studies of these strange ‘zoophytes’, which made liberal use of the microscope, began in 1826 and reached a successful conclusion in the spring of 1827, when he presented his very first scientific paper to the University’s Plinian Society.
These dates coincide with the first appearance of the present model on the market: the instrument was designed by Charles Gould for the firm Cary around 1825, and was certainly on sale by 1826, when its accompanying booklet was mentioned in the Mechanics’ Register. Of the five other surviving microscopes associated with Charles Darwin, four are known to have been acquired later (two in 1831, one each in 1847 and c.1848), and the other cannot be used for studying marine invertebrates.


(thx, mick)
This piece, from Ed Yong, is not at all surprising: America Is Not Ready for Omicron.
America was not prepared for COVID-19 when it arrived. It was not prepared for last winter’s surge. It was not prepared for Delta’s arrival in the summer or its current winter assault. More than 1,000 Americans are still dying of COVID every day, and more have died this year than last. Hospitalizations are rising in 42 states. The University of Nebraska Medical Center in Omaha, which entered the pandemic as arguably the best-prepared hospital in the country, recently went from 70 COVID patients to 110 in four days, leaving its staff “grasping for resolve,” the virologist John Lowe told me. And now comes Omicron.
Will the new and rapidly spreading variant overwhelm the U.S. health-care system? The question is moot because the system is already overwhelmed, in a way that is affecting all patients, COVID or otherwise. “The level of care that we’ve come to expect in our hospitals no longer exists,” Lowe said.
The real unknown is what an Omicron cross will do when it follows a Delta hook. Given what scientists have learned in the three weeks since Omicron’s discovery, “some of the absolute worst-case scenarios that were possible when we saw its genome are off the table, but so are some of the most hopeful scenarios,” Dylan Morris, an evolutionary biologist at UCLA, told me. In any case, America is not prepared for Omicron. The variant’s threat is far greater at the societal level than at the personal one, and policy makers have already cut themselves off from the tools needed to protect the populations they serve. Like the variants that preceded it, Omicron requires individuals to think and act for the collective good — which is to say, it poses a heightened version of the same challenge that the U.S. has failed for two straight years, in bipartisan fashion.
The main point:
Here, then, is the problem: People who are unlikely to be hospitalized by Omicron might still feel reasonably protected, but they can spread the virus to those who are more vulnerable, quickly enough to seriously batter an already collapsing health-care system that will then struggle to care for anyone — vaccinated, boosted, or otherwise. The collective threat is substantially greater than the individual one. And the U.S. is ill-poised to meet it.
Also from Yong: he recently cancelled his 40th birthday party because of Omicron and wrote about how he thought through the decision.
If someone got sick, I know others could too. A week later, many of my friends will spend Christmas with their own families. At best, a cluster of infections at the birthday party would derail those plans, creating days of anxious quarantine or isolation, and forcing the people I love to spend time away from their loved ones. At worst, people might unknowingly carry the virus to their respective families, which might include elderly, immunocompromised, unvaccinated, partially vaccinated, or otherwise vulnerable people. Being born eight days before Christmas creates almost the perfect conditions for one potential super-spreader event to set off many more.
As has been the case the entire pandemic, our political and public health systems are not equipped to collectively combat this virus, so it falls to individuals to make good choices for our communities. It’s a nearly impossible thing to ask to pandemic-weary folks to focus in again on making good personal choices and even harder to achieve if few are willing to do it, but goddammit we have to try.
From Max Roser at Our World in Data: Our history is a battle against the microbes: we lost terribly before science, public health, and vaccines allowed us to protect ourselves.
Science is the foundation for our success. 150 years ago nobody knew where diseases came from. Or more precisely, people thought they knew, but they were wrong. The widely accepted idea at the time was the ‘Miasma’ theory of disease. Miasma, the theory held, was a form of “bad air” that causes disease. The word malaria is testament to the idea that ‘mal aria’ — ‘bad air’ in medieval Italian — is the cause of the disease.
Thanks to the work of a number of doctors and chemists in the second half of the 19th century humanity learned that not noxious air, but specific germs cause infectious diseases. The germ theory of disease was the breakthrough in the fight against the microbe. Scientists identified the pathogens that cause the different diseases and thereby laid the foundation for perhaps the most important technical innovation in our fight against them: vaccines.
Here’s what vaccines did for us, in three charts:
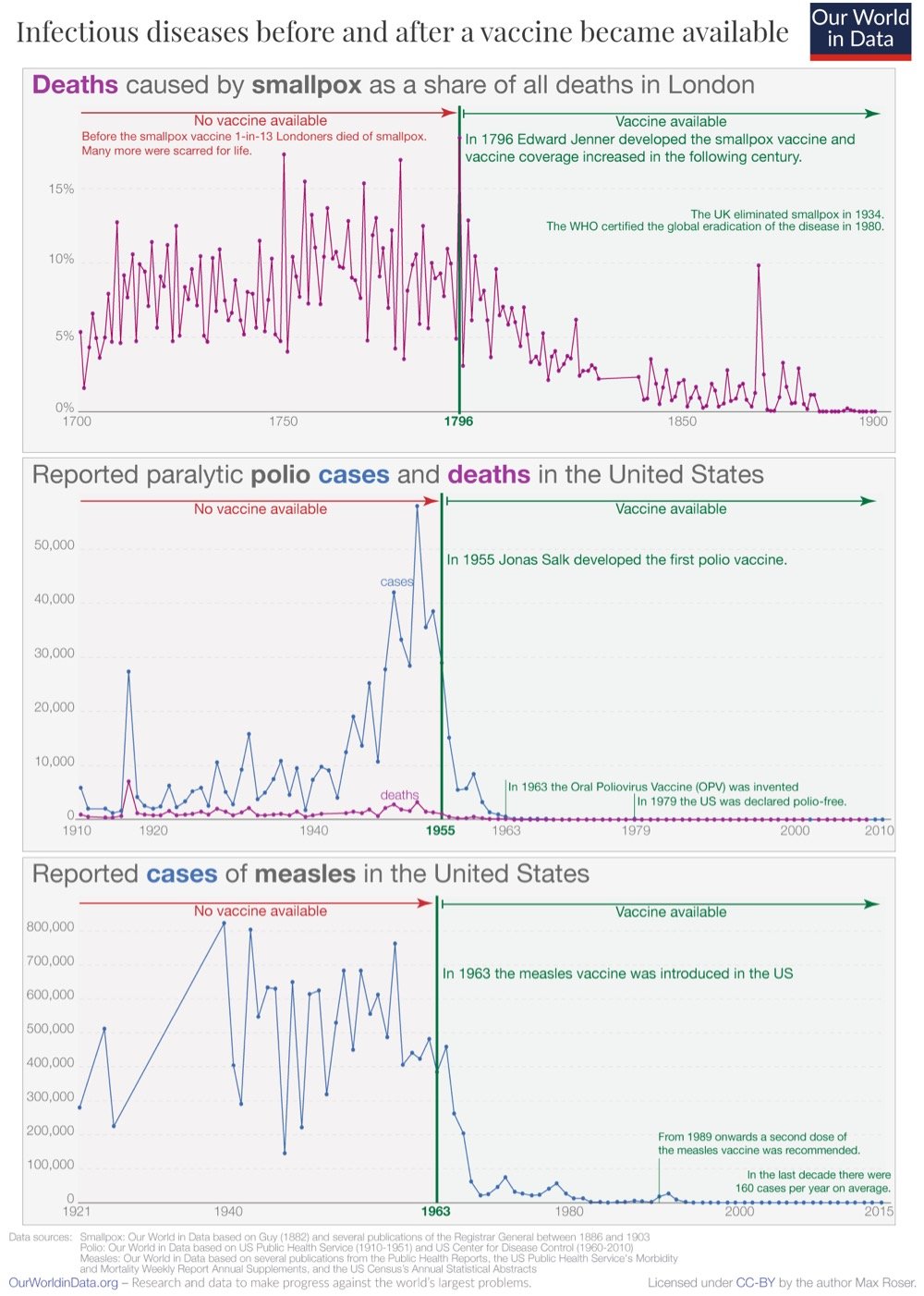
Even among those who accept and understand how good vaccines are at stopping disease, it’s difficult to truly appreciate just how incredible and transformative they have been. By one estimate, vaccines saved between 150 & 200 million lives from 1980 & 2018…and that’s just for smallpox. Covid-19 vaccines have saved hundreds of thousands of lives in Europe and the US in the first year of their availability. Truly a miraculous invention.
Inspired by the second book in Liu Cixin’s excellent Three-Body Problem trilogy, Kurzgesagt made a video about the Dark Forest solution to the Fermi paradox.
Confronted with the seemingly empty universe, humanity faces a dilemma. We desperately want to know if we are alone in the Milky Way. We want to call out and reveal ourselves to anyone watching but that could be the last thing we ever do. Because maybe the universe is not empty. Maybe it’s full of civilizations but they are hiding from each other. Maybe the civilizations that attracted attention in the past were wiped away by invisible arrows. This is the Dark Forest solution to the Fermi paradox.
I have The Dark Forest on the Kindle, so I looked up how this is explained in the book (spoilers, obvs):
“The universe is a dark forest. Every civilization is an armed hunter stalking through the trees like a ghost, gently pushing aside branches that block the path and trying to tread without sound. Even breathing is done with care. The hunter has to be careful, because everywhere in the forest are stealthy hunters like him. If he finds other life-another hunter, an angel or a demon, a delicate infant or a tottering old man, a fairy or a demigod-there’s only one thing he can do: open fire and eliminate them. In this forest, hell is other people. An eternal threat that any life that exposes its own existence will be swiftly wiped out. This is the picture of cosmic civilization. It’s the explanation for the Fermi Paradox.”
Shi Qiang lit another cigarette, if only to have a bit of light.
“But in this dark forest, there’s a stupid child called humanity, who has built a bonfire and is standing beside it shouting, ‘Here I am! Here I am!’” Luo Ji said.
“Has anyone heard it?”
“That’s guaranteed. But those shouts alone can’t be used to determine the child’s location. Humanity has not yet transmitted information about the exact position of Earth and the Solar System into the universe. From the information that has been sent out, all that can be learned is the distance between Earth and Trisolaris, and their general heading in the Milky Way. The precise location of the two worlds is still a mystery. Since we’re located in the wilderness of the periphery of the galaxy, we’re a little safer.”
That’s the basic idea, but there’s more to it…you should watch the video or, even better, read the series — I’ve read the entire trilogy twice and this makes me want to read it again! (I loved the Drive Easter egg towards the end of the video. Well played.)
In this entertaining, informative, and charmingly goofy video, Dr. Kevin Hainline tells us all about the James Webb Space Telescope. The JWST is a bigger and better version of the Hubble Space Telescope and will allow scientists to peer deeper into the universe and farther back in time than ever before.
Listen, science is hard! Engineering is hard! It’s difficult to figure out how to build an incredibly sensitive infrared detector that you have to cram together on the back of a giant, foldable, gold covered mirror, sitting on a delicate, tennis-court-sized parasol, that can survive a rocket launch! It’s hard stuff!
And hundreds and hundreds of people around the world have been working on it together. JWST is the single most complicated science project human beings have ever attempted. But it’s been worth it. Because we want to discover the earliest galaxies in the universe, and clouds on other planets, and baby star-forming regions, and debris disks around stars, and weird dwarf galaxies, and supermassive black holes!
It’s been in development for almost thirty years and everyone is really ready for it! The James Webb Space Telescope is about to change astronomy. Get ready for discovery!
I am ready and excited! The JWST is currently set to launch no earlier than Dec 24, 2021. You can follow the progress of the launch here.
See also Looking back in time with the James Webb Space Telescope (60 Minutes) and 29 Days on the Edge. Oh and scientists have been working on this project for 20 years and are (understandably) really nervous about what happens with the launch.
For the first time in human history, a spacecraft has flown through the Sun’s corona to collect data and capture samples (and, crucially, exited safely).
During the flyby, Parker Solar Probe passed into and out of the corona several times. This is proved what some had predicted — that the Alfvén critical surface isn’t shaped like a smooth ball. Rather, it has spikes and valleys that wrinkle the surface. Discovering where these protrusions line up with solar activity coming from the surface can help scientists learn how events on the Sun affect the atmosphere and solar wind.
Six panels of images taken from inside a coronal streamer. They appear grayish with white streaks showing particles in the solar wind.
At one point, as Parker Solar Probe dipped to just beneath 15 solar radii (around 6.5 million miles) from the Sun’s surface, it transited a feature in the corona called a pseudostreamer. Pseudostreamers are massive structures that rise above the Sun’s surface and can be seen from Earth during solar eclipses.
Passing through the pseudostreamer was like flying into the eye of a storm. Inside the pseudostreamer, the conditions quieted, particles slowed, and number of switchbacks dropped — a dramatic change from the busy barrage of particles the spacecraft usually encounters in the solar wind.
For the first time, the spacecraft found itself in a region where the magnetic fields were strong enough to dominate the movement of particles there. These conditions were the definitive proof the spacecraft had passed the Alfvén critical surface and entered the solar atmosphere where magnetic fields shape the movement of everything in the region.
The first passage through the corona, which lasted only a few hours, is one of many planned for the mission. Parker will continue to spiral closer to the Sun, eventually reaching as close as 8.86 solar radii (3.83 million miles) from the surface. Upcoming flybys, the next of which is happening in January 2022, will likely bring Parker Solar Probe through the corona again.
The video above provides a great overview of the origins, objectives, and motivations for the mission.
The YouTube channel Two Minute Papers enthusiastically shares the findings from scientific papers about technology: computing, graphics, AI, robotics, etc. Recently they reviewed this paper on simulating the growth of large-scale plant ecosystems based on real-world forestry and botany research. From the paper’s abstract:
In this paper we describe a multi-scale method to design large-scale ecosystems with individual plants that are realistically modeled and faithfully capture biological features, such as growth, plant interactions, different types of tropism, and the competition for resources. Our approach is based on leveraging inter- and intra-plant self-similarities for efficiently modeling plant geometry. We focus on the interactive design of plant ecosystems of up to 500K plants, while adhering to biological priors known in forestry and botany research.
What that means, as they show in the video, is that you can watch these incredibly detailed time lapse videos of forests developing over time in a realistic way. So cool. This kind of thing always reminds me of favorite childhood thing, Al Jarnow’s Cosmic Clock. (via waxy)
Mathematics isn’t the most obviously cinematic academic discipline out there, but it is one that the movies (and to a lesser extent television) have repeatedly tried to understand, or in some cases, used to goose up a vaguely science-y story. Unsurprisingly, mathematicians often become sticklers for detail in such high-profile depictions of what they do, and a good or bad portrayal can become famous or infamous.
My friend Jordan Ellenberg, a math professor at the University of Wisconsin-Madison, is also an expert in translating math to popular audiences, in his books and sometimes on screen. In this video, he takes a look at some popular representations of math in TV and the movies, and tries to explain what’s going on, including what the filmmakers do well or not so well.
Good Will Hunting’s use of math is famously bad, and Ellenberg unsurprisingly agrees (although, surprisingly, he had never before seen the movie or even the math scenes in question). Portrayals that get a perhaps-surprisingly high score include The Simpsons (which includes several former mathematicians among its writers) and Jurassic Park — Jeff Goldblum pulls off a passable explanation of chaos theory while also eerily accurately capturing the slightly-creepy vibe of a neurotic academic asked to describe what he studies to a layperson. “He was the one who I most felt might have spent a long time studying mathematicians and truly trying to give off a mathematician vibe,” says Ellenberg.
One thing I love is Ellenberg’s attention to how each of the on-screen mathematicians write (if they do any writing themselves at all, rather than ponder something that’s already been written by a character offscreen) — the connection between math and writing is so powerful, and math is one of the great remaining repositories of manuscript culture (even as it’s also taken on computers and machines, like everything else).
Ellenberg also adds that the most important thing a movie about mathematics can do is to convey to the audience that being a mathematician is something real, ordinary people still do, rather than being just a bunch of old dead men wearing robes.
How do you steer a bike? You turn the handlebars to the left to go left, correct? Actually, you don’t: you turn the handlebars to the right to go left…at least at first. And also? Bikes don’t even need riders to remain upright…they are designed to steer themselves.
If you’d like to play around with your own bicycle geometries, try this web app for analyzing bicycle dynamics.
Last week, a worrisome variant of SARS-CoV-2 burst into the public consciousness: the Omicron variant. The concern among scientists and the public at large is substantial, but it is unfortunately going to take a few weeks to figure out whether those concerns are warranted. For a measured take on what we know now and what we can expect, read these two posts by epidemiologist Dr. Katelyn Jetelina (as well as this one on vaccines).
B.1.1.529 has 32 mutations on the spike protein alone. This is an insane amount of change. As a comparison, Delta had 9 changes on the spike protein. We know that B.1.1.529 is not a “Delta plus” variant. The figure below shows a really long line, with no previous Delta ancestors. So this likely means it mutated over time in one, likely immunocompromised, individual.
Of these, some mutations have properties to escape antibody protection (i.e. outsmart our vaccines and vaccine-induced immunity). There are several mutations association with increased transmissibility. There is a mutation associated with increased infectivity.
That sounds bad but again, we presently do not have enough information to know for sure about any of this. As Jetelina concludes in one of the posts:
We still have more questions than answers. But we will get them soon. Do not take Omicron lightly, but don’t abandon hope either. Our immune systems are incredible.
None of this changes what you can to do right now: Ventilate spaces. Use masks. Test if you have symptoms. Isolate if positive. Get vaccinated. Get boosted.
This Science piece by Kai Kupferschmidt also provides a great overview about where we’re at with Omicron, without the sensationalism.
Whether or not Omicron turns out to be another pandemic gamechanger, the lesson we should take from it (but probably won’t) is that grave danger is lurking in that virus and we need to get *everyone* *everywhere* vaccinated, we need free and ubiquitous rapid testing *everywhere*, we need to focus on indoor ventilation, we need to continue to use measures like distancing and mask-wearing, and we need to keep doing all of the other things in the Swiss cheese model of pandemic defense. Anything else is just continuing our idiotic streak with this virus of fucking around and then finding out. (via jodi ettenberg & eric topol)
In this video, whale scientist Nan Hauser tells the story about how a humpback whale she was swimming with saved her from what she calls “the largest tiger shark I’ve ever seen”. It turns out this is not atypical behavior for humpbacks — they’re one of the nicest animals in the sea or on land and have been known to rescue animals from other species from predators.
First-person accounts of animals saving other animals are rare. Robert Pitman, a marine ecologist with the US National Oceanic and Atmospheric Administration, describes a pivotal encounter he witnessed in Antarctica in 2009. A group of killer whales washed a Weddell seal they were attacking off an ice floe. The seal swam frantically toward a pair of humpbacks that had inserted themselves into the action. One of the huge humpbacks rolled over on its back and the 180-kilogram seal was swept up onto its chest between the whale’s massive flippers. When the killer whales moved in closer, the humpback arched its chest, lifting the seal out of the water. And when the seal started slipping off, the humpback, according to Pitman, “gave the seal a gentle nudge with its flipper, back to the middle of its chest. Moments later, the seal scrambled off and swam to the safety of a nearby ice floe.”
Is this behavior in humpbacks altruistic or even compassionate? Or is it “just” instinct?
So are humpbacks compassionate? Scientists, Sharpe tells me, shy away from using the same descriptors we use for humans. “What is exciting about humpbacks is that they are directing their behavior for the benefit of other species,” he says. “But there’s no doubt there are important differences between human compassion and animal compassion.” When I pose the same question to Pitman he concurs. “No editor is going to let me use the word compassion. When a human protects an imperiled individual of another species, we call it compassion. If a humpback whale does so, we call it instinct. But sometimes the distinction isn’t all that clear.”
Somehow, I missed the teaser trailer for Don’t Look Up a couple months back, but the official trailer just came out yesterday. Directed by Adam McKay (The Big Short, Vice) and starring Leonardo DiCaprio & Jennifer Lawrence (and Meryl Streep, Jonah Hill, Mark Rylance, Cate Blanchett, Tyler Perry, and Timothée Chalamet), Don’t Look Up is a comedy about what happens when scientific fact (in the form of a planet-killing comet) slams into the fantasy worlds of politics and entertainment media. Just because you can’t spin Newton’s laws of motion doesn’t mean you can’t try!
Nothing, absolutely nothing whatsoever, about this movie is related to current events, nope, no sir. *sobbing intensifies* (I love disaster movies and will 100% see this even though it will probably be completely enraging.)
I have been a fan of how things are made videos since my Mister Rogers and Sesame Street days, so I was not expecting to be so surprised watching the video above about how bowling balls are made. It’s a ball — how complicated could it be? Well, it turns out that modern bowling balls contain an asymmetric weight block in the middle that looks a little like a car’s starter. Weird, right?
As I started to wonder why it would be advantageous to include such a lopsided core in a ball you want to roll predictably down a lane, I noticed YouTube’s algorithm doing its job in recommending that I watch Veritasium’s recent video on How Hidden Technology Transformed Bowling, which totally explains the wonky weight block thing:
The weight blocks are wonky in a precise way. They’re designed to cause the ball to contact the lane over more of the surface of the ball, giving it more traction once it hits the unoiled part of the lane, which is desirable for expert bowlers looking for a wicked hook. So cool! (thx, mick)
Update: Brendan Koerner wrote a piece for Wired several months ago about Mo Pinel, who revolutionized bowling with the asymmetric cores described in the video above.
Pinel toured Faball’s factory and examined a freshly made core that the company used in its Hammer brand. It had a symmetrical and unexciting shape — the center looked like a lemon, and there were two convex caps of equal size on either side. In a moment that has now passed into ball-design legend, Pinel grabbed the core, which was still soft because the polyester had yet to cure, and sliced off the ends with a palette knife. Then he smooshed the caps back on into positions that were slightly askew, so that the contraption now looked like a Y-wing fighter from Star Wars.
The ball that contained this revamped core, the Hammer 3D Offset, would become Pinel’s signature achievement. “That ball sold like hotcakes for three years, where the average life span of a ball was about six months,” says Del Warren, a former ball designer who now works as a coach in Florida. “They literally couldn’t build enough of them.” In addition to flaring like few other balls on the market, the 3D Offset was idiot-proof: The core was designed in such a way that it would be hard for a pro shop to muck up its action by drilling a customer’s finger holes incorrectly, an innovation that made bowlers less nervous about plunking down $200 for a ball.
(via @danhwylie)

A group of epidemiologists have analyzed all 25 James Bond movies to assess the risks Bond encounters on his travels around the globe.
The result is a highly entertaining, tongue-in-cheek short paper in the journal Travel Medicine and Infectious Disease. The paper details 007’s exposure risk to infectious agents during his global travels, covering everything from foodborne pathogens to ticks and mites, hangovers and dehydration from all those martinis, parasites, and unsafe sex.
Some of the findings include that 007 should wash his hands more often, frequently risks dehydration and heatstroke due to improper hydration, often engages in unsafe sex with partners whose sexual histories are unknown to him, and endangers his sexual partners (“27.1% of them died shortly after sex”). My favorite finding is the speculation that Bond contracted Toxoplasmosis1 from a cat in From Russia With Love and that’s why he engages in risky behavior all the time:
The biggest stretch in Graumans et al.’s analysis is that of feline-borne Toxoplasmosis, a parasite carried by cats. Those who contract the parasite tend to exhibit reckless behavior, such as mice losing their fear of cats. Bond engages in all manner of reckless behavior, and the authors suggest he may have contracted the parasite from Ernst Stavro Blofeld’s fluffy white Persian cat (featured in both From Russia With Love and Spectre). The possibility is admittedly far-fetched, but isn’t that the essence of a good Bond film?
Using samples of chopped-down wood left behind by Viking explorers at their settlement in Newfoundland and known chemical markers of powerful solar storms in 993 AD, a group of scientists has determined the exact timing of the first-known visit of Europeans to North America: 1021 AD. If you’re keeping score at home, that’s 471 years before Columbus.
A team of scientists looked at wood found at the L’Anse aux Meadows Viking site. In three cases the trees had been physically cut down, and moreover, they were clearly cut with metal tools — Vikings had metal implements at the time, but indigenous people did not. The wood was all from different trees (one was fir, and another juniper, for example). The key parts here are that the wood was all from trees that had been alive for many decades, and all had their waney edge intact as well.
The scientists extracted 127 samples from the wood, and 83 rings were examined. They used two methods to secure dates. The first was to compare the amount of carbon-14 in each ring with known atmospheric amounts from the time. This gives a rough date for the waney edge of the wood. They also then looked for an anomalous spike in carbon-14 in an inner ring, knowing this would have come from the 993 A.D. event, and then simply counted the rings outward from there to get the date of the waney edge.
In all three samples the waney edge was dated to the same year: 1021 A.D. This would be incredibly unlikely to occur at random.
Outstanding science. It’s incredible how much of a time machine these analysis tools are. There’s so much we don’t know about people who lived 1000 years ago, but it’s astounding that we know anything at all, particularly precise dates like this.
Update: From this Ars Technica piece, some more information on the precision of the dating:
Based on the development stages of certain cells in the waney layer, Dee, Kuitems, and their colleagues say that one of the trees was cut down in the spring, while another was cut down in the summer or fall. The third tree’s final season couldn’t be identified because the cells had been damaged by a conservation treatment, but the results suggest that the Norse cut down these trees within a few months of each other in 1021.
That lends additional support to the other evidence that the Norse only stayed in Newfoundland for a few years.
“One would imagine the dates would have been different if the occupation period of the site was very long,” Dee told Ars. “However, the fact all three of our samples produced the same date does not, of course, mean the site was only occupied for one year. It may indeed have been occupied longer. But I think it is true to say our results support a short occupation.”
For the last nine months, NASA’s Perseverance rover has been rolling around on Mars taking photos and doing science. It’s also been recording audio of its environment with a pair of microphones and in this video, a pair of NASA scientists share some of those recordings and what we might learn about Mars from them.
This is one of my absolute favorite sounds. This is the sound of a helicopter flying on Mars. We used this sound to actually understand the propagation of sound in general through the Martian atmosphere, and it turns out that we were totally wrong with our models. The Martian atmosphere can propagate sound a lot further than we thought it could.
And surprisingly for me, that’s my friend Nina in the video! (We eclipse-chased together in 2017.) I knew she was working on the rovers but didn’t know she was going to pop up in this video I found on Twitter this morning. Fun!
The fossil record has provided us with so much information about plants, animals, and organisms that lived hundreds, thousands, millions, and even billions of years ago. But we are actually only seeing evidence of a tiny fraction of the species that lived then and even for those we do know about, there’s often much we still don’t know. Traditionally, dinosaurs have been depicted as drab and often terrible lizards but recent finds of soft tissues (skin, feathers, etc.) and an increased sense of imagination based on our current vibrant biodiversity has people thinking differently about how they looked and behaved.
In trying to explain what you’re about to see here, I cannot improve upon the Dr. Adrian Smith’s narration at the beginning of this video:
But sometimes I think the most useful thing I can do as a scientist is to point the fancy science cameras at some moths flapping their wings in front of a purple backdrop. I mean, whose day isn’t going to be better after watching a pink and purple rosy maple moth flying in super slow motion? This is a polyphemus moth, a gigantic species of silk moth. What you are seeing, like all the rest of the clips in this video, was filmed at 6,000 frames per second.
Most of the moths in the video are delightfully fuzzy and chonky — if these moths were birds, they’d be birbs. Shall we call them mopfs?
The rest of Smith’s AntLab videos are worth looking through — I’ve previously posted about his slow motion videos here. (via aeon)
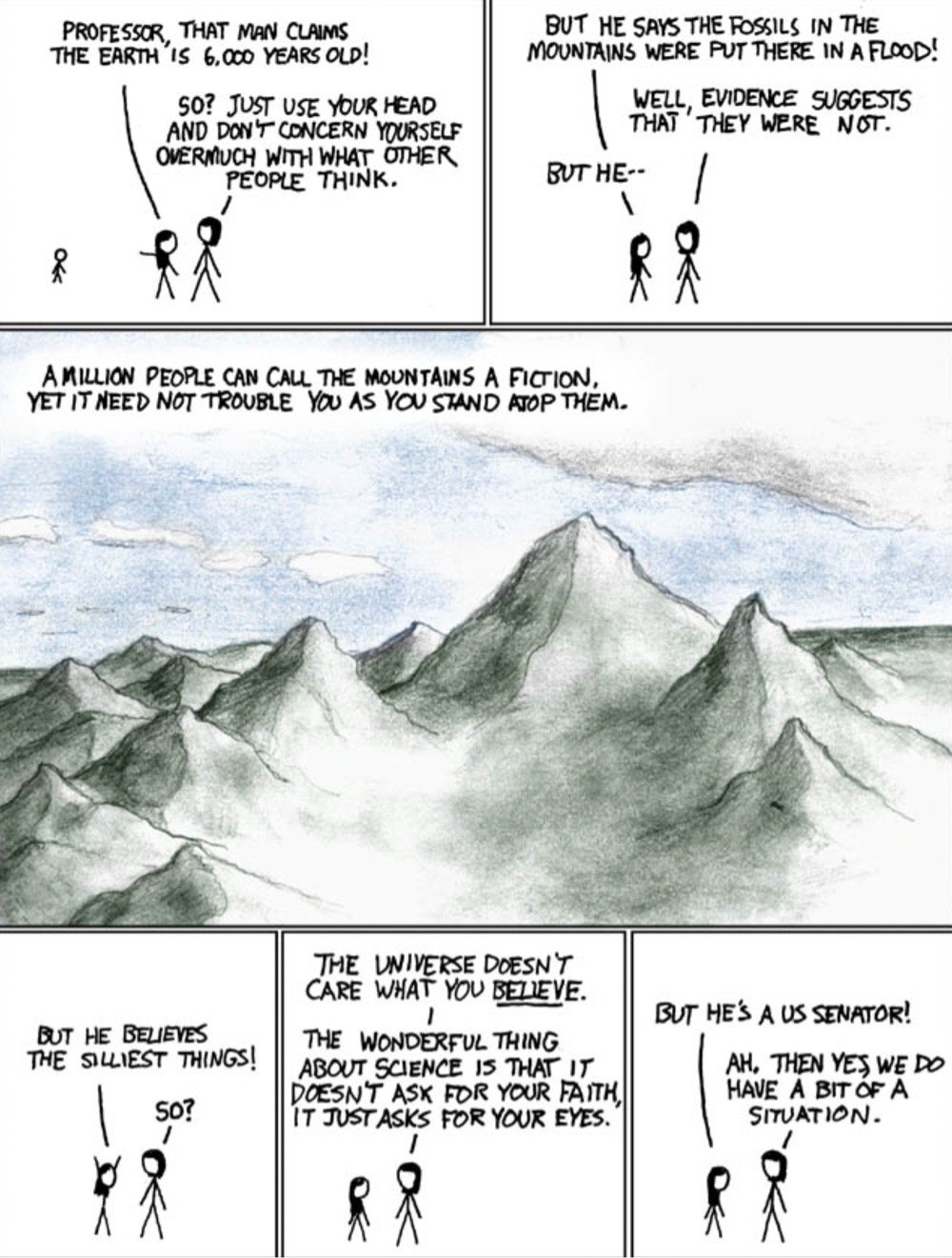
From 2019 to 2021, a small Spanish football team was renamed Flat Earth FC, both as a publicity stunt and because club president Javi Poves couldn’t understand how water “curves”.
“Football is the most popular sport and has the most impact worldwide, so creating a club dedicated to the flat earth movement is the best way to have a constant presence in the media,” said Poves earlier this year. “Flat Earth FC is the first football club whose followers are united by the most important thing, which is an idea.”
The club’s crest is now a circular image of the earth, pressed flat on to all kits, and fans are encouraged to spark regular conversations in their pursuit of answers from the powers that be. The team mascot? An astronaut. It’s a radical move, but the club is bringing in supporters from afar. “It’s really amazing to be part of this amazing movement,” says Flat Earth player Mario Cardete. “I think it’s more than a club.”
During the pandemic, the club also became anti-mask and anti-vax — because conspiracy theories come in price-saving 3-packs, I guess? Poves resigned in late 2020 and the club was renamed and then purchased by a larger club to become their reserve team. The Earth remains round.
So let’s say, for the sake of argument and against all scientific evidence to the contrary, the Earth was flat instead of being an oblate spheroid. What would life on a flat Earth be like? Well for one thing, gravity would present some challenges. From a 2018 piece by Doug Main at the Columbia Climate School:
People who believe in a flat Earth assume that gravity would pull straight down, but there’s no evidence to suggest it would work that way. What we know about gravity suggests it would pull toward the center of the disk. That means it would only pull straight down at one point on the center of the disk. As you got increasingly far from the center, gravity would tug more and more horizontally. This would have some strange impacts, like sucking all the water toward the center of the world, and making trees and plants grow diagonally, since they develop in the opposite direction of gravity’s pull.
And even more than that, gravity would tend to pull a flat disc shape back into a spheroid, so absent an intense spinning force (for which there is zero evidence) or some other completely unknown effect, a flat Earth couldn’t even exist:
For Earth to take the shape of a flat disk in the first place, gravity — as we know it — must be having no effect. If it did, it would soon pull the planet back into a spheroid.
A flat Earth would also likely not have a magnetic field (or at least one that is scientifically possible), meaning no atmosphere:
Deep below ground, the solid core of the Earth generates the planet’s magnetic field. But in a flat planet, that would have to be replaced by something else. Perhaps a flat sheet of liquid metal. That, however, wouldn’t rotate in a way that creates a magnetic field. Without a magnetic field, charged particles from the sun would fry the planet. They could strip away the atmosphere, as they did after Mars lost its magnetic field, and the air and oceans would escape into space.
Oh and no tectonic plates, volcanos, mountains, etc. Or GPS. Or weather. Or satellites. Or different night skies in, say, South Africa and Denmark. Or the Sun behaving the way it does in respect to the Earth. Or air travel. Or plant and animal life as it exists presently. To suppose a flat Earth also supposes that physics doesn’t explain our observable universe the way in which it reliably and comprehensively does. The simplest, best evidence for a round Earth is that we’re here living on it in the manner in which we are living on it.
See also What If the Earth Suddenly Turned Flat?, Flat Earthers and the Double-Edged Sword of American Magical Thinking, and Flat Earthers Listening to Daft Punk.
Train wheels do not sit completely flat on the tracks — they’re designed with a slight taper that increases the stability of the train and allows the train to go around curves without any of the wheels skidding. In this short video, Tadashi Tokieda explains how those conical wheels keep trains on track.
See also Richard Feynman’s explanation of this and this science project at Scientific American. (via the prepared)
Ed Yong: We’re Already Barreling Toward the Next Pandemic. The US is throwing too little money at high-tech, ultimately private sector solutions but much of the problem comes down to our underfunded public health system and “profoundly unequal society”.
“To be ready for the next pandemic, we need to make sure that there’s an even footing in our societal structures,” Seema Mohapatra, a health-law expert at Indiana University, told me. That vision of preparedness is closer to what 19th-century thinkers lobbied for, and what the 20th century swept aside. It means shifting the spotlight away from pathogens themselves and onto the living and working conditions that allow pathogens to flourish. It means measuring preparedness not just in terms of syringes, sequencers, and supply chains but also in terms of paid sick leave, safe public housing, eviction moratoriums, decarceration, food assistance, and universal health care. It means accompanying mandates for social distancing and the like with financial assistance for those who might lose work, or free accommodation where exposed people can quarantine from their family. It means rebuilding the health policies that Reagan began shredding in the 1980s and that later administrations further frayed. It means restoring trust in government and community through public services. “It’s very hard to achieve effective containment when the people you’re working with don’t think you care about them,” Arrianna Marie Planey, a medical geographer at the University of North Carolina at Chapel Hill, told me.
Within the past 50 years, the global community has solved two huge problems that had the potential to harm every person on Earth. Smallpox once killed 30% of the people who contracted the disease but through the invention of an effective, safe vaccine and an intense effort that began in the 1960s, smallpox was completely eradicated by 1980. In the 1980s, scientists discovered a hole in the ozone layer that protects the Earth from UV radiation; further depletion would have caused major problems with the world’s food supply and an epidemic of skin cancer. Forty years later, we’ve virtually eliminated the chemicals causing the depletion and ozone losses have stabilized and have recently shown improvement.
So how did we do it? The short video above talks through each of challenges, how they were met (science + politics + a bit of luck), and how we might apply these lessons to the big problems of today (climate emergency, the pandemic).
Bored of dying from Covid-19, Americans have dreamed up a more entertaining way to mortally wound themselves: the milk crate challenge. Wired asked structural engineer Dr. Nehemiah Mabry (who explained the different types of bridges to us earlier in the year) to explain the physics behind the challenge and why you shouldn’t attempt it. (via @pomeranian99)
In one of their most popular videos in awhile, kottke.org favorite Kurzgesagt tells us about something I’d never heard of before: giruses. These giant viruses have only been discovered within the last 20 years and are so large and contain so much genetic material that maybe they are actually alive?
Hidden in the microverse all around you, there is a merciless war being fought by the true rulers of this planet, microorganisms. Amoebae, protists, bacteria, archaea and fungi compete for resources and space. And then there are the strange horrors that are viruses, hunting everyone else. Not even being alive, they are the tiniest, most abundant and deadliest beings on earth, killing trillions every day. Not interested in resources, only in living things to take over. Or so we thought.
It turns out that there are giant viruses that blur the line between life and death — and other viruses hunting them.
It may seem like sometimes that with the pandemic, we’re back to square one. With the much more contagious Delta variant in play and an increasing number of breakthrough infections, the efficacy of these vaccines that we thought were amazing maybe aren’t? (Or maybe we just need to readjust our expectations?) But in terms of what these vaccines were specifically developed for — reducing & preventing severe disease and death — they are still very much doing their job. Just take a look at this graph from a White House Covid-19 press briefing yesterday:
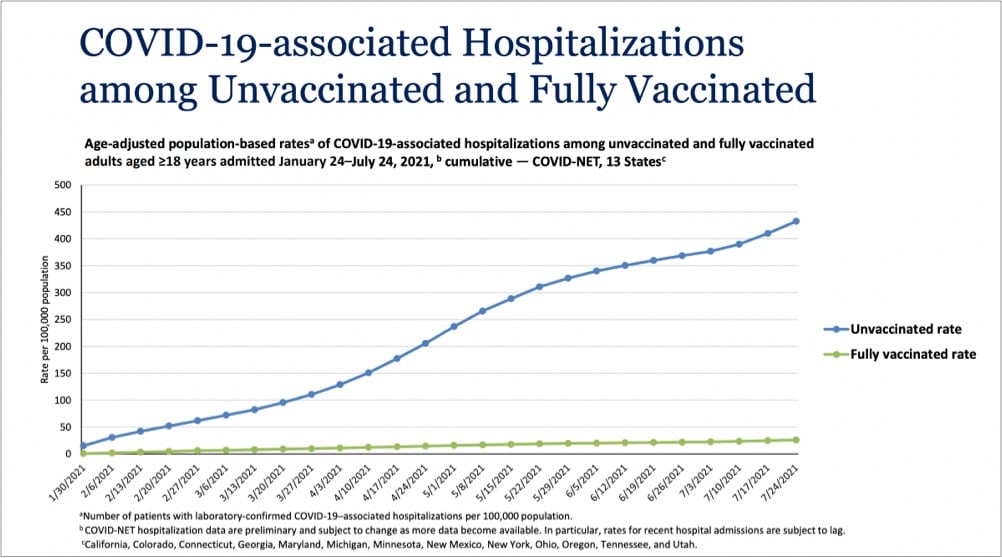
Even with Delta endemic in the country, the vaccines are providing extraordinary protection against infections severe enough to land folks in the hospital. In a recent CDC study of infections and hospitalizations in Los Angeles County, they report that on July 25, the hospitalization rate of unvaccinated people was 29.2 times that of fully vaccinated persons. 29 times the protection is astounding for a medical intervention. These vaccines work, we’re lucky to have them, and we need to get as many people worldwide as we can vaccinated as quickly as we can. Period.
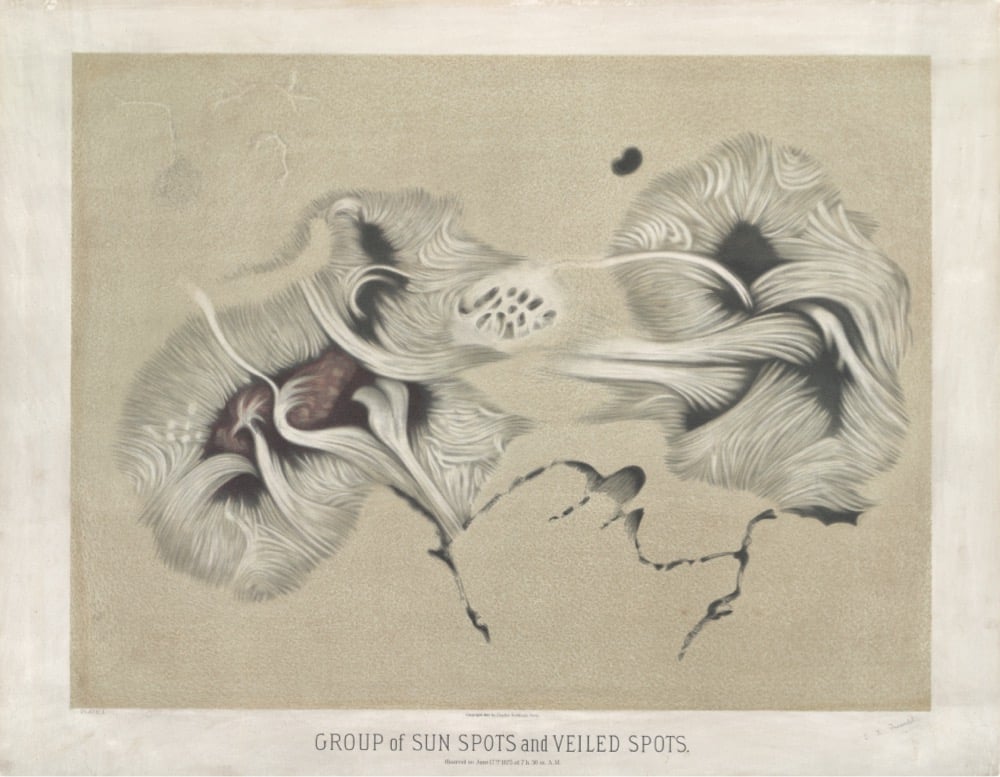
I love this post from the NYPL comparing astronomical drawings by E.L. Trouvelot done in the 1870s to contemporary NASA images.
Trouvelot was a French immigrant to the US in the 1800s, and his job was to create sketches of astronomical observations at Harvard College’s observatory. Building off of this sketch work, Trouvelot decided to do large pastel drawings of “the celestial phenomena as they appear…through the great modern telescopes.”
He made drawings of Saturn, Jupiter, aurora borealis, the Milky Way, and more. Here’s his incredible drawing of sun spots compared to a recent image of the Sun’s surface:
And his drawing of a solar eclipse compared to a recent image:


Check out the post for more examples of Trouvelot’s work.
For The Atlantic, Katherine Wu writes about the difficulty of communicating how vaccines work and how they protect individuals and communities from disease: Vaccines Are Like Sunscreen… No, Wait, Airbags… No, Wait…
Unfortunately, communal benefit is harder to define, harder to quantify, and harder to describe than individual protection, because “it’s not the way Americans are used to thinking about things,” Neil Lewis, a behavioral scientist and communications expert at Cornell, told me. That’s in part because communal risk isn’t characteristic of the health perils people in wealthy countries are accustomed to facing: heart disease, stroke, diabetes, cancer. Maybe that’s part of why we gravitate toward individual-focused comparisons. Slipping into a pandemic-compatible, population-based frame of mind is a big shift. In the age of COVID-19, “there’s been a lot of focus on the individual,” Lewis told me. That’s pretty at odds “with how infection works.”
As someone who has struggled with analogizing the virus & vaccines, I was nodding my head a lot while reading this. Something I’ve noticed in recent years that Wu didn’t get into is that readers desire precision in metaphors and analogies, even though metaphor is — by definition! — not supposed to be taken literally. People seem much more interested in taking analogies apart, identifying what doesn’t work, and discarding them rather than — more generously and constructively IMO — using them as the author intended to better understand the subject matter. The perfect metaphor doesn’t exist because then it wouldn’t be a metaphor.
One of the many effects of human-driven climate change is that, on average, the bodies of animals are getting smaller — birds, fish, deer, frogs, rodents, insects. And these changes could have large and unpredictable consequences.
“That’s the problem with human-driven climate change. It’s the rate of change that’s just orders of magnitude faster than what the natural world has had to deal with in the past. Size is really important to survival, and you can’t just change that indefinitely without consequence. For one thing, I don’t think it’s feasible that species are going to be able to continue to get smaller and maintain things like a migration from one hemisphere to another.”
And since smaller bodies can hold fewer eggs, they result in fewer offspring, and a lower population size in the long run. For amphibians who need to keep their skin wet in order to breathe, shrinking can mean higher chances of drying out in a drought because their bodies absorb and hold smaller quantities of water.
But the more concerning consequences have to do with how this could destabilize relationships between species. Because shrinking plays out at different rates for different species, predators might have to eat more and more of shrinking prey, for example, throwing a finely-tuned ecosystem off balance.
Newer posts
Older posts
Socials & More